I’d like to talk with you about an anecdotal experience I recently had with a client.
I had a runner come to me who was experiencing knee pain. If I had stopped in my assessment at simply looking at the function of the knee, I would have missed the primary driver of the compensation pattern. Because I linked the relationship of the Anterior Kinetic Chain, and the core cylinder, I was able to correlate an internal oblique issue to the medial knee. It’s not uncommon for ligaments to compensate for the burden when muscular function is impaired. My ability to move beyond the obvious to a deeper level of inquiry – which is what we learn in Dynamic Neuromuscular Assessment™ Seminars – allowed me to get to the more profound root issue for my client.
Anatomy and kinesiology are two disciplines that give clarity to the interdependence of the structure and movement of the body.
Anatomy is the language used to describe the parts. These parts then fit together into systems that synergistically make up the whole organism.
Kinesiology is the language of movement. Through kinesiology, anatomy is given a context. If the language of movement is a symphony, the role of anatomy is to describe the source of each note of music.
Anatomy charts provide the fundamental foundation for understanding the names of bones, joints, ligaments, tendons, muscles, fascia, and so forth – the structure. Kinesiology then defines how each aspect of structure works together to create movement.
One of my teachers, early on in my career, imparted the importance of the breath, movement, and structure as being interdependent.
Movement is a translator to how the structure organizes, movement can’t lie. When the body is experiencing pain, the brain reorganizes movement so that we move around our pain instead of through it. This avoidance is a compensation to keep us in a perceived safe zone. As practitioners, our ability to see deviation in movement is paramount to assisting our clients. Often the walking gait is the lens through which we look during assessment. The 5 Primary Kinetic Chains provide a map of the gait.
The use of color in The 5 Primary Kinetic Chains illustrations imparts upon the teacher/student or practitioner/client, how the body organizes during movement. The kinetic chain charts further define how the body organizes in the optimal manner during gait. Why the gait? The gait is universal to human movement. From birth, our nervous system is prewired for developmental movement with the intention to get us upright and biped. If you have interest in a more in-depth conversation on the walking gait, see my blog on the Master Template. The synergistic organization, or sequential muscular activation, gives context to efficient movement and helps us to identify potential dysfunctional relationships that may not be obvious at first impression to the client or practitioner.
When the synergistic organization of our movement becomes less than optimal, or compensated, the result are over and underworked players. Synergistic dominance is the relationship between these over and under worked players. As a practitioner it is useful to have reference tools – like The 5 Primary Kinetic Chains Poster Set or Desktop Edition to help us dig deeper into the function and dysfunction presented by our clients.
Please leave a comment below about a powerful experience you had either as a client or practitioner where you or they went beyond the obvious to the profound!
Please note this particular series of blogs will describe each of the four muscles and their relationship to the five principal actions described in the charts of The 5 Primary Kinetic Chain Poster Set I’ve developed. This is Part Two of four. You can find Part One on the Piriformis here.
Introduction:
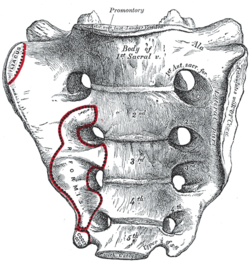
The sacrum, or sacred bone, is unique in the body. Mystics regard the sacrum as the focal point for kundalini, the spiraling energy that rises from the root through the crown. This triangular shaped bone provides the base of support for the spinal column.
The sacrum articulates with the pelvis through the sacral iliac joint, SIJ. The kinetic energy of ground force reaction moves from the feet engaging the earth, up through the legs, into the pelvis. The energy crosses through the pelvis into the sacrum and up through the axis of the spine. The manner by which this energy moves into and through the axis of the spine defines our ability to respond to ground force reaction.
There are four important muscles that act directly on the sacrum.
Posterior Surface:
multifidus/sacrospinalis
gluteus maximus
These four high level muscles often are not engaged with their task of stabilizing the sacrum through a spectrum of movement. When we look at the function of these four muscles, and the various movement they are involved in, there is a trend we see in most people’s presentation that are seeking therapeutic intervention.
The anterior surface muscles are often up-regulated. These muscles are over worked and do not respond appropriately. One of the flavors of synergistic dominance is when one group of fibers becomes up-regulated, those dominant fibers then down-regulate the function of that muscle over its spectrum of movement.
The posterior surface muscles are often down-regulated and are not available to respond appropriately to movement.
The relationship of how these four muscles work together in coordination changes over the spectrum of movement. The 5 Primary Kinetic Chains have unique Principal Actions that inform the sequence of movement. This series of essays will describe each of the four muscles and their relationship to the five principal actions.
Ilacus:
The iliacus is a large primary muscle of the pelvis that attaches to the bowl of the pelvis, the iliac fossa. This muscle has a large surface area as it fans across the inner bowl of the pelvis. The multiple direction of these fibers give them advantage over a range of functions.
As the fibers of the iliacus come off the pelvic bowl, they knit together multiple structures of the pelvis. Fibers attach to the anterior sacral ligaments, the sacrum, the psoas, and the lessor trochantor of the femur.
Looking at the web of connective tissue between the iliacus, the psoas, the anterior sacral ligaments, and the direct attachment on the body of the sacrum, it becomes clear that the iliacus has a profound effect on the sacrum.
The fibers of the iliacus are joined by the fibers of the psoas. Together they create a common tendon attachment on the lesser trochanter. This makes the iliacus and the psoas an important synergistic pair, yet they have some different roles in movement.
The psoas is a multi-segmented muscle. The psoas crosses multiple joints of the lumbar spine. Muscles that cross multiple joints have an important role as a stabilizer during the work production phase of movement. The shorter fibered muscles that cross one joint are the hard working prime mover. The important distinction here is that the psoas is acting on the lumbar spine while the iliacus is acting on the pelvis. When these two muscles are not playing well as individuals, or as a synergistic pair, the result is a destabilized lumbar-pelvis.
The iliacus is considered one of the more common up-regulated muscles. The bracing, or shortening action of an up-regulated iliacus, affects the sacroiliac joint, SIJ.
As the iliacus acts on the ilium, the relationship of a neutral SIJ becomes altered. The movement of the sacrum is self-limiting by the SIJ, while the ilium has more freedom to move around the sacrum creating a mobile/stable relationship. Hip rotation, hip hiking, and hip flare are relationships to sagittal, coronal, and transverse plane movement. The iliacus is involved in these movements even if it isn’t the driver.
Concentric Actions of The Iliacus:
Sagittal ~ hip flexion, ilium rotation, & sacral flexion
Transverse ~ hip external rotation, ilium flare & sacral downward/upward rotation on an oblique axis
The Iliacus and The 5 Primary Kinetic Chains:
Intrinsic ~ Breath
The iliacus is considered an extrinsic muscle of the pelvic floor. When you consider movement of the ilium, sacrum, and hip, the pelvic floor is involved.
The following two scenarios are common presentations:
Spinal Wave:
The iliacus is a participant in the spinal wave during the breath cycle.
An up-regulated iliacus is the action of the exhalation phase thereby affecting the inhalation phase of the breath. This is a relationship of reciprocal inhibition.
Pelvic Floor:
The iliacus attaches on the bowl of the pelvis creating an extrinsic boundary. An up-regulated iliacus partners with the pelvic floor. During the inhalation phase of the breath, the pelvic floor’s action is eccentric lengthening. An up-regulated pelvic floor loses this ability.
Deep Longitudinal ~ Shock Absorption
An up-regulated iliacus interferes with the kinetic wave of shock absorption. The up-regulated iliacus is a bracing strategy for the SIJ. Compression in the SIJ functionally acts as an abutment to the kinetic wave of ground force reaction.
The body’s appropriate response to the kinetic wave of shock absorption is to counter with the push reflex. Imagine stepping off the curb. The hip must descend so that the foot can meet the ground. This is an eccentric action of the quadrates lumborum, the QL. An up-regulated iliacus down-regulates the push reflex.
Lateral ~ Axial Stability
The adductor magnus, a lateral kinetic chain subsystem muscle, needs to play well with the iliacus. The adductor magnus is a synergist with the adductor longus. The iliacus is synergist with the adductor longus.
During the transition phases of the gait, mid stance, late stance, propulsion, and shift, this synergistic pair action is eccentric lengthening. This lengthening is storing elastic energy that will be released in the swing phase of the gait.
The lateral kinetic chain is in contralateral relationship with the anterior spiral kinetic chain: stance/swing. This movement requires stability across the anterior surface of the sacrum. The iliacus and contralateral piriformis become functional synergists during the swing phase of the gait. Looking at these kinds of contralateral relationships is an important aspect in movement assessment.
The iliacus and piriformis pictured here are in ipsilateral relationship. When the iliacus and piriformis are in contralateral relationship they create a functional X across the anterior surface of the sacrum.
Posterior Spiral ~ Generation of Stored Elastic Energy
The coiling of the thoracolumbar fascia acts on the sacrum and the SIJ. The hip is extending and externally rotating. The iliacus is actively engaged in eccentric lengthening, or is a functional opposite.
An up-regulated iliacus is going to down-regulate the coiling action of the posterior spiral kinetic chain. This is important when looking at the posterior surface muscles that act on the sacrum. Often, multifidus/sacrospinalis and gluteus maximus are down-regulated and need to get back into the equation for sacral stability.
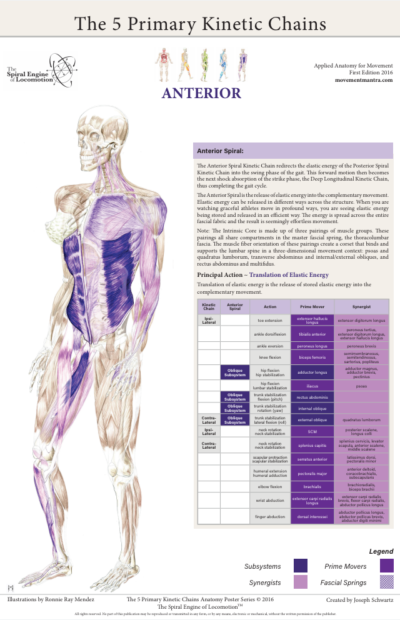
Anterior Spiral ~ Translation of Stored Elastic energy
The iliacus is a powerful hip flexor. An up-regulated iliacus will look for recruits to assist in hip flexion during the swing phase of the gait. The common players the body looks to recruit are the psoas, tensor fasciae latea, rectus femoris, sartorius, and all the adductors.
The anterior spiral pairs with the contralateral lateral kinetic chain. At the moment when hip extension translates into hip flexion, the iliacus and the contralateral piriformis are in functional synergist relationship. This creates stability across the anterior sacrum during shock absorption.
Remote Relationships:
The body starts to look for recruitments to assist an up-regulated and fatigued muscle/s. One common recruitment pattern are muscles in contralateral pairs. The pectoralis minor and the iliacus are common up-regulated muscles, they work together in the contralateral shoulder to hip relationship of the anterior spiral.
Manual Therapy Application:
One important aspect of any manual intervention is to ask the body directly if the modality is appropriate. This can be verified by doing a little bit of release. Go back to the relationship and take notice. Did the response change in a favorable way? If it did, then the release technique was appropriate. If it did not, then the nervous system needs something else to restore the coordination.
Here are a few strategies I regularly employ when working with an up-regulated iliacus.
Strain Counter Strain:
This is a one of my favorite go to techniques. It is gentle and effective. There is little risk to further irritation of an up-regulated iliacus. The lessor trochanter, the common tendon junction and the bowl of the pelvis are good entry points for this gentle technique.
Belted Pelvis:
This active bilateral release can have a dramatic positive effect in the SIJ. The belt puts the SIJ in compression while the bilateral activation of internal/external rotation resets the receptors. The therapist can approach the release in two ways. One is to use feedback pressure to activate the balance between internal and external rotation. The other is to use bilateral pressure on both piriformi to reset the muscle spindles.
Active Muscle Spindle:
This is a technique that resets the muscle spindles interpretation of muscle length. Support clients leg with thigh vertical, leg horizontal. Have the client hold their leg in place to accurately access the common tendon junction near the bowl of the pelvis. The placement of the practitioners fingers should be such that there is zero visceral impingement. Once appropriate contact is made, the clientslowly extends the leg and draws back to the starting position.
Pin and Stretch:
This flossing technique is a mixed bag. It can either be highly effective or over stimulates the nervous system. Ask the body if it is appropriate to the client’s presentation.
Conclusion:
When assessing the players involved with sacral stability, ask if the identified players can cooperate with each other. Getting all the players back on the same team make for a happy sacrum.
Glossary:
Concentric activation ~ The muscle fibers are shortening; the muscle attachments are moving toward one another.
Eccentric activation ~ The muscle fibers are lengthening; the muscle attachments are moving away from one another.
Synergist ~ Muscles that work together during movement.
Functional Opposite ~ Muscles that work opposite to one another. One muscle is lengthening while the other is shortening.
Up-Regulated ~ An overstimulated muscle that is compensating for other muscle/s that are not participating. Often the muscle will become overworked and fatigued and unable to respond appropriately.
Down-Regulated ~ An under stimulated muscle. The function is impaired and unable to respond appropriately.
Reciprocal Inhibition ~ When a muscle/s is contracting, the opposite muscle/s must be lengthening. If the opposite muscle/s are unable to lengthen, being up-regulated for example, then that will functionally inhibit the muscle that is contracting.
*Please note this particular series of blogs will describe each of the four muscles and their relationship to the five principal actions described in the charts of The 5 Primary Kinetic Chain Poster Set I’ve developed. This is the first in a series of four posts. You can find the second post on the Iliacus here.
Introduction to the Sacrum:
The sacrum, or sacred bone, is unique in the body. Mystics regard the sacrum as the focal point for kundalini, the spiraling energy that rises from the root through the crown. This triangular shaped bone provides the base of support for the spinal column.
The sacrum articulates with the pelvis through the sacral iliac joint, SIJ. The kinetic energy of ground force reaction moves from the feet engaging the earth, up through the legs, into the pelvis. The energy crosses through the pelvis into the sacrum and up through the axis of the spine. The manner by which the energy moves into and through the axis of the spine defines our ability to respond to ground force reaction.
There are four important muscles that act directly on the sacrum.
Posterior Surface: multifidus/sacrospinalis & gluteus maximus
These four high level muscles often are not engaged with their task of stabilizing the sacrum through a spectrum of movement. When we look at the function of these four muscles, and the various movement they are involved in, there is a trend we see in most people’s presentation that are seeking therapeutic intervention.
The anterior surface muscles are often up-regulated. These muscles are over worked and do not respond appropriately. One of the flavors of synergistic dominance is when one group of fibers becomes up-regulated, those dominant fibers then down-regulate the function of that muscle over its spectrum of movement.
The posterior surface muscles are often down-regulated and are not available to respond appropriately to movement.
The relationship of how these four muscles work together in coordination changes over the spectrum of movement. The 5 Primary Kinetic Chains have unique principal actions that inform the sequence of movement. This series of essays will describe each of the four muscles and their relationship to the five Principal Actions I’ve described in the 5 Primary Kinetic Chains poster set.
Piriformis:
The piriformis is a flat, pyramidal shaped muscle that runs from the anterior surface of the sacrum to the greater trochanter of the femur. The manner by which the muscle fans across the broad surface of the sacrum is somewhat similar to the subscapularis attaching to the scapula. The piriformis is an external rotator of the femur; the subscapularis is an internal rotator of the humerus, thereby making them functional opposites.
Many people have challenges due to the structure and function of their piriformis. Approximately one in 5 of us have piriformis anomalies (Read more here). Those that have this are often grouped into a category of “piriformis syndrome,” a pattern of up-regulated piriformis that irritates and compresses the nerve bundles, the sciatica nerve, that pass through the muscle.
People that have this presentation are often challenged by common movement triggers. Prolonged sitting, driving, and — for some — simply walking, is enough to exacerbate the pressure of the muscle acting on the nerve.
Concentric Actions of The Piriformis:
Sagittal ~ hip extension & sacral flexion
Coronal ~ hip abduction & sacral downward/upward rotation (limited by SIJ gap)
Transverse ~ hip external rotation & sacral downward/upward rotation on an oblique axis
The Piriformis and The 5 Primary Kinetic Chains:
Intrinsic ~ Breath
The relationship between the piriformis and the pelvic floor is often a good starting point for evaluation. The following two scenarios are common presentations:
Spinal Wave:
The piriformis is a participant in the spinal wave during the breath cycle.
An up-regulated piriformis is the action of the exhalation phase thereby affecting the inhalation phase of the breath.
Pelvic Floor:
The sacral tuberous ligament, and the obturator internus help make up the extrinsic boundaries of the pelvic floor. The piriformis is a synergist to the obturator internus making it an easily recruitable option for an up-regulated pelvic floor.
Deep Longitudinal ~ Shock Absorption
An up-regulated piriformis interferes with the kinetic wave of shock absorption. The up-regulated piriformis is a bracing strategy for the SIJ. Compression in the SIJ functionally acts as an abutment to the kinetic wave of ground force reaction.
The body’s appropriate response to the kinetic wave of shock absorption is to counter with the push reflex. Imagine stepping off the curb. The hip must descend so that the foot can meet the ground. This is an eccentric action of the quadrates lumborum, the QL. An up-regulated piriformis down-regulates the push reflex.
The peroneal nerve, a division of the sciatic nerve, innervates the subsystem muscles of the deep longitudinal kinetic chain. An up-regulated piriformis that compresses the peroneal nerve will affect the peroneus muscles and the short head of the bicep femoris. When these subsystem muscles are unable to respond appropriately, the compensation is joint compression strategies that will move up the kinetic chain.
Lateral ~ Axial Stability
The gluteus medius, a lateral kinetic chain subsystem muscle, needs to play well with the piriformis. The piriformis is both a synergist and functional opposite to actions of the gluteus medius.
The gluteus medius attaches to the pelvis with a broad fan-like orientation of fibers. The action includes abduction of the hip, and internal and external rotation of the femur. This is significant because some fibers act as synergists and others act as functional opposites. Often, select fibers of an up-regulated gluteus medius will functionally down-regulate the other fibers. This contributes to an up-regulated piriformis.
The lateral kinetic chain is in contralateral relationship with the anterior spiral kinetic chain: stance / swing. This movement requires stability across the anterior surface of the sacrum. The contralateral iliacus and the piriformis become functional synergists during the swing phase of the gait.
The iliacus and piriformis pictured here are in ipsilateral relationship. When the iliacus and piriformis are in contralateral relationship they create a functional X across the anterior surface of the sacrum.
Posterior Spiral ~ Generation of Stored Elastic Energy
The coiling of the thoracolumbar fascia acts on the sacrum and the SIJ. The hip is extending and externally rotating. The piriformis is a synergist to the gluteus maximus, a posterior spiral subsystem muscle and sacral stabilizer.
Potentially any muscles in the posterior spiral kinetic chain could be in a synergistic dominance relationship.
Posterior spiral kinetic chain is paired with the contralateral deep longitudinal kinetic chain. The push leads the strike; the piriformi are in an alternating activation.
Anterior Spiral ~ Translation of Stored Elastic energy
The anterior spiral pairs with the contralateral lateral kinetic chain. At the moment when hip extension translates into hip flexion, the ipsilateral iliacus and the piriformis are in functional synergist relationship.
Remote Relationships:
The body starts to look for recruitments to assist an up-regulated and fatigued muscle. One common recruitment pattern is muscles that have similar fibril orientation. The lateral pterigoid is a common jaw remote relationship.
Manual Therapy Application:
One important aspect of any manual intervention is to ask the body directly if the modality is appropriate. This can be verified by doing a little bit of release. Go back to the relationship and take notice. Did the response change in a favorable way? If it did, then the release technique was appropriate. If it did not, then the nervous system needs something else to restore the coordination.
There are few strategies I regularly employ when working with an up-regulated piriformis.
Strain Counter Strain:
This is a one of my favorite go to techniques. It is gentle and effective. There is little risk to further irritation of an up-regulated piriformis.
Belted Pelvis:
This active bilateral release can have a dramatic positive effect in the SIJ. The belt puts the SIJ in compression while the bilateral activation of internal/external rotation resets the receptors. The therapist can approach the release in two ways. One is to use feedback pressure to activate the balance between internal and external rotation. The other is to use bilateral pressure on both piriformi to reset the muscle spindles.
Pin and Stretch:
This flossing technique is a mixed bag. It can either be highly effective or over stimulate the nervous system. Ask the body if it is appropriate to the client’s presentation.
Conclusion:
When assessing the players involved with sacral stability, ask if the players can cooperate with each other. Getting all the players back on the same team make for a happy sacrum.
Glossary:
Concentric activation ~ The muscle fibers are shortening; the muscle attachments are moving toward one another.
Eccentric activation ~ The muscle fibers are lengthening; the muscle attachments are moving away from one another.
Synergist ~ Muscles that work together during movement.
Functional Opposite ~ Muscles that work opposite to one another. One muscle is lengthening while the other is shortening.
Up-Regulated ~ An overstimulated muscle that is compensating for other muscle/s that are not participating. Often the muscle will become overworked and fatigued and unable to respond appropriately.
Down-Regulated ~ An under stimulated muscle. The function is impaired and unable to respond appropriately.
People want to know how the anatomy poster series, The 5 Primary Kinetic Chains, differ from other anatomy posters, specifically Anatomy Train’s Myofascial Meridians.
Let’s start with a little back ground.
I started my exploration of the field of somatics, movement as a therapy, and bodywork strategies, back in 1986. I had suffered a severe injury in a rock climbing fall. I hyper flexed my ankle (dorsal) and broke my talus, the load bone between the leg and the foot. The talus is a unique skeletal bone as it doesn’t have any muscular attachments, rather the talus is held in place by ligaments and the articulation of neighboring joints. I was very fortunate that I didn’t kill the blood supply to the bone and I made phenomenal progress in healing.
I found a great chiropractor that facilitated both manual therapy and movement progressions. I ended up being a case study at Stanford University for the degree of recovery that I realized. I still have a limitation of dorsal flexion, but overall I am very lucky that I met this healer to guide me in what would become my life vocation.
I dabbled with bodywork for a few years before getting formal training in 1992, when I enrolled at Alive & Well, The Institute of Conscious BodyWork in San Anselmo. The school was owned by Jocelyn Oliver and David Weinstock. Jocelyn had pioneered an approach for massage therapy integrating manual muscle testing from Touch For Health. The work progressed and elements of Applied Kinesiology began to integrate as well.
I found myself completely intrigued and absorbed with this approach of changing the response of the nervous system and the structure follows. I sought out as much knowledge as I could about muscle testing, motor control, and strategies in approaching structural change. I was always on the lookout for books that would further my understanding. In my research, I found Dr. George Goodheart’s book, Applied Kinesiology Synopsis. This was the bible of AK and the source to resolve musculoskeletal dysfunction. In a college bookstore, I found another publication, Vernon Brooks’ book, The Neural Basis of Motor Control. I excitingly shared this with my colleagues and teachers. I wanted to understand how cueing in the nervous system with muscle testing could facilitate rapid change in the ability for the structure to respond differently via muscle testing. The Neural Basis of Motor Control helped to answer that question. Both books are out-of-print, but with a little effort can still be found.
A few years later I moved from California to the Austin, TX area. I quickly gained a reputation for the skill sets I had as a bodyworker. Through a series of referrals from the area’s naturopathic doctors, I found I had a group of practitioners that wanted to learn the approach I used in manual muscle testing combined with structural corrections.
Over the course of years, I developed my own hybrid format from the foundation I learned at Alive & Well. I was seeing patterns in movement. I thought of them as maps. I could trace the maps, find the dysfunctional component, correct that component and reinsert it back into the map.
In 2001 or perhaps 2002, Tom Myers came to Austin to teach his new course Anatomy Trains. One of the students in my group took that course. He said to me, “Joseph, you’re not going to believe this, Tom talks about the connection of movement and fascia like you do. Look at these drawings.” When I looked at them, I saw something very similar to the maps I was sharing with my students. I was intrigued; I was not alone in the discoveries I was making.
Several years later Myers’ posters were published. I purchased a set of posters and would refer to them with clients. The myofascial meridians are an excellent map of how structure links together. Practitioners, students and clients have all benefited from their visual reference.
Fast forward to today.
Here is a look at how these two poster series are different yet complementary. The myofascial meridians are looking through the lens of structure. The unification of the fascia, the compartments that bind and wrap the body, including muscles, tendons, ligaments and joints, even the bones themselves (tensegrity and the double bag theory are important concepts every bodyworker should be versed in). Kinetic chains are looking through the lens of movement. The kinetic chains explore how the neuromuscular activation acts on the fascia compartments and how these activations connect, creating a synergistic whole.
Now let’s look at what sets The 5 Primary Kinetic Chains poster series apart.
The 5 Primary Kinetic Chains are based on the movement of the contralateral gait. Our nervous system is hard wired for developmental movement to learn to walk and run so that we can hunt and evade predators, survival.
The 5 Primary Kinetic Chains have roots in the concept of the core subsystems which was introduced by Dr. Andry Vleeming. These core subsystems, slings, or transmission systems, do not operate in isolation from the rest of the musculosketal system. The whole fascia network is involved in movement. A kinetic chain is the synergistic relationship of how structure is responding to movement.
The illustrations of The 5 Primary Kinetic Chains are beautifully done and give a three-dimensional feeling of movement. Each kinetic chain is color coded with three levels of depth that represent the three categories of the muscular relationships. The bold color are the subsystems: the major players in Vleeming’s core slings. The mid-tones are the prime movers: the muscles that have positional advantage to do the most work. The lighter tones are the synergists: the helper muscles. Every part is working in concert to create balanced and efficient movement.
To make it easier for use in a learning or clinical setting the muscle charts are organized joint by joint.
Another feature of the poster series is that each chart has a Principal Action. I refer to this as the Master Template. These five Principal Actions are present in all integrated movement. Our breath, relationship to gravity and shock absorption, dynamic stability through the axis, and ability to store elastic energy — and then translate that elastic energy — is a holistic approach to movement.
The Myofascial Meridians and The 5 Primary Kinetic Chains complement each other, and together unify a more complete understanding of integrated movement.
The Five Primary Kinetic Chains rely on a fundamental principle: efficient movement requires the integration of a stable yet dynamic foundation so that the body can generate the power needed for locomotion.
The Anterior Spiral is a culmination of everything that we’ve discussed previously. As such, let’s review how the previous four kinetic chains have worked together to get us to this final kinetic chain.
The Intrinsic system is related to the nervous system and breath. The breath is a barometer for our movement. How our breath is integrated with our movement determines how our nervous system responds. If we move in a manner by which the movement breathes the body, the sympathetic nervous system can remain down-regulated, thus giving us access to refined motor control. If instead our breath reaches the threshold of cardiovascular distress, or we are holding our breath out of bracing or fear, our sympathetic nervous system becomes up-regulated and arms the body with a flood of chemistry.
One of the markers for stress tolerance is the capacity to return from an aroused sympathetic nervous system back to a calm parasympathetic down-regulated state of being. A large percentage of our population is stuck in an up-regulated sympathetic nervous system. This is a stress reaction that results in inflammation in the body contributing to decreased healing and regenerative ability. As a result, it is becoming popular to “train” the vagus nerve — the tenth cranial nerve — to experience arming and disarming the nervous system.
There are some very good modalities to specifically address an up-regulated sympathetic nervous system. Our personal practice is one way we can take responsibility for our stress levels. Tia Chi, Qi Gung, Shamatha Meditation, and Yoga are but a few examples. I personally find getting acupuncture to be very much a sattvic practice. I go very deep into meditation as I’m observing the energy shifts in my subtle body. For people that are attracted to manual therapy, Cranial Sacral Therapy is a wonderful way to engage the nervous system and the breathing apparatus. Nervous system health very well may start with the subtle aspects of how the cranial sutures are integrating with breath and movement.
The Deep Longitudinal Kinetic Chain is about how we interact with gravity and shock absorption. Our bodies are under a constant compressive force. The energy of the compressive force changes as movement and locomotion further generates kinetic energy. The energy of our bodies in motion must be absorbed and translated. The energy is distributed across the fascial fabric of our bodies.
This energy becomes a dynamic platform, the Lateral Kinetic Chain. The Lateral KC provides dynamic stability so that the appendicular skeleton has a foundation from which to work off. Without this foundation, the body would be at a disadvantage in generating stored elastic energy.
In developmental movement, the reflexive motor learning that is hard wired into our nervous system, we see that the movements are all about creating dynamic stability with the intention of getting us upright and using a bi-ped strategy of locomotion, the walking gait.
With an established dynamic platform, we have the capacity to store and release elastic energy. Elastic energy is stored in the tissues in two modes: lengthening or stretching and coiling or compressing. When tissues lengthen or stretch, the fascia’s elasticity stores energy. This would be like stretching a rubber band across your finger and releasing it; the rubber bands soars across the room. Likewise, winding up the rubber band on a model airplane illustrates the second mechanism of storing and releasing elastic energy. As the rubber band coils tightly, energy is stored; more coiling equates to more compression that stores energy to release.
The Posterior Spiral Kinetic Chain is the avenue the body uses to coil elastic energy into the fascial springs that perpetuate the energy of the walking gait. The body is utilizing both modalities (lengthening and coiling) for activating the fascial fabric to generate stored elastic energy. As the Posterior Spiral KC is coiled to release that energy, the ipsilateral anterior spiral is lengthening. It is a coiling of one side of the body and a lengthening on the opposite. The body is utilizing both pathways simultaneously, to generate stored elastic energy.
The Anterior Spiral completes the gait cycle. Elastic energy up to this point has been stored into the tissues, and now the body is poised to do something with that energy. The body will now translate the stored elastic energy into the complementary movement. The forward motion generated by the push of the posterior spiral is realized through the leg swing of the anterior spiral.
The ability to effectively store and release elastic energy is paramount to athletic performance. In the video, notice the quality of movement this athlete displays. The timing of arm drive and leg drive, the depth of absorbing kinetic energy, and how the explosive energy increases with each shock absorption phase. Her movement is brilliant and demonstrates healthy integrated kinetic chains at work.
The 5 Primary Kinetic Chains working together create an integrated whole. If one or more of the components are unable to engage, then we need to isolate the issue and through motor learning, reengage and integrate back into the whole. The kinetic chain charts are meant to be a map for inquiry, as we explore who is playing and who is not, the charts can help us to discern what disengaged players need to get back in the game.
The charts in the Five Primary Kinetic Chains Anatomy Poster Series outline a primary physiological principle in movement: bones, joints, ligaments, tendons, muscles and fascia do not work in isolation. They work synergistically to create movement.
When movement is balanced and efficient, the players are all cooperating with each other. If movement is out of balance and inefficient, the result is compensation in the structure. This maladaptive compensation follows some specific physiological principles.
The first of these principles, synergistic dominance, is when one synergistic component of the structure is compensating for another synergistic component. More specifically, one component is overworked or up-regulated in relationship with another synergist that is underworked or down-regulated.
Synergistic dominance can show up over a spectrum of compensatory strategies. It can show up locally or globally. A local example would be the relationship of a muscle to itself. The distal end of a muscle can be up-regulated for a down-regulated proximal end of the same muscle. Synergist dominance will also show up when multiple muscles are working together. For example, hip flexion has several muscles that work synergistically. The iliacus, psoas, tensor fasciae latea, rectus femoris, adductor longus, and sartorious are the major contributors to hip flexion. If one of these muscles is up-regulated, that can functionally down-regulate the others.
Synergistic dominance also shows up globally. Kinetic chains, the manner in which the musculoskeletal system organizes itself, is not merely a local occurrence. Kinetic chains organize across the entire fascial fabric. The lateral kinetic chain provides a good example of global synergistic dominance. Throughout the dynamic platform of the stance phase of the gait, the ankle, pelvis, torso, and neck all need to play well together. If they are unable to do so, then one player will take over doing the job of the player unable to engage. Single leg stance is a great global assessment protocol to discern synergistic dominance of the lateral kinetic chain.
Synergistic dominance can also show up in kinetic chains that work in unison. For example, during the gait cycle, the posterior spiral kinetic chain is paired with the opposite deep longitudinal kinetic chain. Likewise, the lateral kinetic chain is paired with the opposite anterior spiral kinetic chain. These pairings of kinetic chains have an interdependent relationship. One relies on the other in the efficiency of storing and releasing elastic energy. If one chain has a dysfunctional component, it is going to have an effect on the other, they are in a synergistic relationship.
The other side of the synergist coin is the functional opposite. Muscles that work in opposition to one another rely on a principal called reciprocal inhibition. Reciprocal inhibition defines that the agonist, contracts or shortens, as the opposite, the antagonist, must lengthen. Simply, if one muscle is shortening then the other must be lengthening. If the muscle that should be lengthening is unable to do so, the effect is that the muscle that needs to shorten becomes down-regulated. It is unable to overcome the up-regulated muscle, as it can’t compete.
Functional opposites happen across kinetic chains just as synergists do. The foundation of understanding synergistic dominance builds the prerequisite for investigating functional opposites. As movement evolves, essentially there are two things happening: some tissues are shortening while others are lengthening.
The charts included in The 5 Primary Kinetic Chains posters provide a map for synergistic relationships. By mapping the synergists, one can then decode functional opposites. This is a very useful learning tool as well as a visual reference for your clients and patients.
All movement leads to adaptation creating compensation.
The law of adaptation: The organism adapts to its environment regardless of outcome. The nervous system does not differentiate whether an adaptation is beneficial or not.
I have seen several clients over the years, seasoned yoga practitioners, that had a similar root problem with different outcomes. The problem was a recruitment pattern with the toes. The instruction to “floint” the foot is to flex the toes while pointing the forefoot. This is also known as “Barbie Feet.”
Compensation in the toes creates global compensation patterns. These patterns occur along front and back kinetic chains. Kinetic chains can be understood as muscles that link together to create integration. When one muscle becomes inhibited, the chain is broken. This results in some muscles that are overworked, and others that are underworked. When the toe flexors become dominate, two different patterns can emerge.
Patterns of inhibition along the same kinetic chain as the toe flexors, along the front of the body are known as synergists. One client had pain just below her hip joint in the front of her thigh. The hip flexors were inhibited by her toe flexors. Every step she took exasperated the problem. Another client had pain in the back of her thigh. She had patterns of inhibition along the back of the body. This pattern is the functional opposite to the toe flexors.
There are other groups of people that have kinetic chain imbalances due to toe flexor dominance. People that wear high heels and/or flip flops are also high risk.
Whatever activity we regularly do, will unknowingly create undesirable movement patterns. Fortunately, undesirable patterns are learned behavior. Thus, they can be unlearned and replaced by a more desirable pattern.