There seems to be lot of “dysfunctional psoas causing back pain” articles. I’d like to offer another viewpoint.
Say a person does have an inhibition in their psoas. What effects would that have on posture?
The short answer is: a general facilitation along the anterior kinetic chain. The body doesn’t like to be in a position it cannot stabilize. If it is weak in an action such as flexion, the body will move more into flexion, which gives the illusion of being in a safe position.
This position then affects the ability of the hamstring to act on the ischial tuberosity. How do you think the lumbar is going to respond when it does not have the reciprocal muscles balancing extension?
The next question that we should be asking is why is the psoas inhibited in the first place? Is that the causation or a symptom of something else?
Lots of questions, and each person has their unique answer.
Looking deeper into causation instead of chasing symptoms is a good practice.
Don’t just treat what you find, look deeper. Peel away the layers.
Ask for next level factors. It could be structural. It could be physiological. It could be emotional/cognitive. There are environmental factors as well as habitual influences that could be in play. How we work and how we move are all considerations as well.
We are complex human beings, not just muscles and a nervous system.
The psoas is involved in posture, stability, and breath. Read more about the “Mighty Psoas” here.
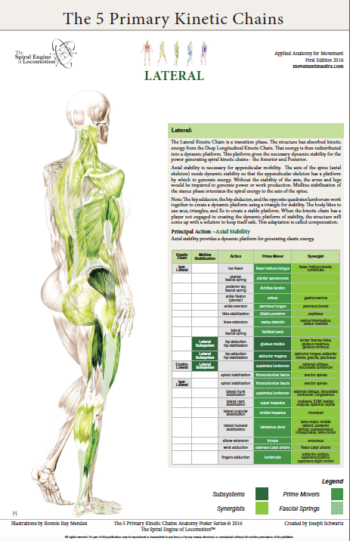
Please note this particular series of blogs will describe each of the four muscles and their relationship to the five principal actions described in the charts of The 5 Primary Kinetic Chain Poster Set I’ve developed. This is Part Two of four. You can find Part One on the Piriformis here.
Introduction:
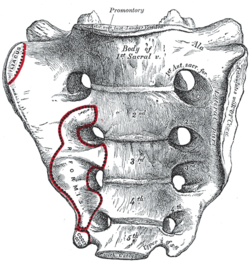
The sacrum, or sacred bone, is unique in the body. Mystics regard the sacrum as the focal point for kundalini, the spiraling energy that rises from the root through the crown. This triangular shaped bone provides the base of support for the spinal column.
The sacrum articulates with the pelvis through the sacral iliac joint, SIJ. The kinetic energy of ground force reaction moves from the feet engaging the earth, up through the legs, into the pelvis. The energy crosses through the pelvis into the sacrum and up through the axis of the spine. The manner by which this energy moves into and through the axis of the spine defines our ability to respond to ground force reaction.
There are four important muscles that act directly on the sacrum.
Posterior Surface:
multifidus/sacrospinalis
gluteus maximus
These four high level muscles often are not engaged with their task of stabilizing the sacrum through a spectrum of movement. When we look at the function of these four muscles, and the various movement they are involved in, there is a trend we see in most people’s presentation that are seeking therapeutic intervention.
The anterior surface muscles are often up-regulated. These muscles are over worked and do not respond appropriately. One of the flavors of synergistic dominance is when one group of fibers becomes up-regulated, those dominant fibers then down-regulate the function of that muscle over its spectrum of movement.
The posterior surface muscles are often down-regulated and are not available to respond appropriately to movement.
The relationship of how these four muscles work together in coordination changes over the spectrum of movement. The 5 Primary Kinetic Chains have unique Principal Actions that inform the sequence of movement. This series of essays will describe each of the four muscles and their relationship to the five principal actions.
Ilacus:
The iliacus is a large primary muscle of the pelvis that attaches to the bowl of the pelvis, the iliac fossa. This muscle has a large surface area as it fans across the inner bowl of the pelvis. The multiple direction of these fibers give them advantage over a range of functions.
As the fibers of the iliacus come off the pelvic bowl, they knit together multiple structures of the pelvis. Fibers attach to the anterior sacral ligaments, the sacrum, the psoas, and the lessor trochantor of the femur.
Looking at the web of connective tissue between the iliacus, the psoas, the anterior sacral ligaments, and the direct attachment on the body of the sacrum, it becomes clear that the iliacus has a profound effect on the sacrum.
The fibers of the iliacus are joined by the fibers of the psoas. Together they create a common tendon attachment on the lesser trochanter. This makes the iliacus and the psoas an important synergistic pair, yet they have some different roles in movement.
The psoas is a multi-segmented muscle. The psoas crosses multiple joints of the lumbar spine. Muscles that cross multiple joints have an important role as a stabilizer during the work production phase of movement. The shorter fibered muscles that cross one joint are the hard working prime mover. The important distinction here is that the psoas is acting on the lumbar spine while the iliacus is acting on the pelvis. When these two muscles are not playing well as individuals, or as a synergistic pair, the result is a destabilized lumbar-pelvis.
The iliacus is considered one of the more common up-regulated muscles. The bracing, or shortening action of an up-regulated iliacus, affects the sacroiliac joint, SIJ.
As the iliacus acts on the ilium, the relationship of a neutral SIJ becomes altered. The movement of the sacrum is self-limiting by the SIJ, while the ilium has more freedom to move around the sacrum creating a mobile/stable relationship. Hip rotation, hip hiking, and hip flare are relationships to sagittal, coronal, and transverse plane movement. The iliacus is involved in these movements even if it isn’t the driver.
Concentric Actions of The Iliacus:
Sagittal ~ hip flexion, ilium rotation, & sacral flexion
Transverse ~ hip external rotation, ilium flare & sacral downward/upward rotation on an oblique axis
The Iliacus and The 5 Primary Kinetic Chains:
Intrinsic ~ Breath
The iliacus is considered an extrinsic muscle of the pelvic floor. When you consider movement of the ilium, sacrum, and hip, the pelvic floor is involved.
The following two scenarios are common presentations:
Spinal Wave:
The iliacus is a participant in the spinal wave during the breath cycle.
An up-regulated iliacus is the action of the exhalation phase thereby affecting the inhalation phase of the breath. This is a relationship of reciprocal inhibition.
Pelvic Floor:
The iliacus attaches on the bowl of the pelvis creating an extrinsic boundary. An up-regulated iliacus partners with the pelvic floor. During the inhalation phase of the breath, the pelvic floor’s action is eccentric lengthening. An up-regulated pelvic floor loses this ability.
Deep Longitudinal ~ Shock Absorption
An up-regulated iliacus interferes with the kinetic wave of shock absorption. The up-regulated iliacus is a bracing strategy for the SIJ. Compression in the SIJ functionally acts as an abutment to the kinetic wave of ground force reaction.
The body’s appropriate response to the kinetic wave of shock absorption is to counter with the push reflex. Imagine stepping off the curb. The hip must descend so that the foot can meet the ground. This is an eccentric action of the quadrates lumborum, the QL. An up-regulated iliacus down-regulates the push reflex.
Lateral ~ Axial Stability
The adductor magnus, a lateral kinetic chain subsystem muscle, needs to play well with the iliacus. The adductor magnus is a synergist with the adductor longus. The iliacus is synergist with the adductor longus.
During the transition phases of the gait, mid stance, late stance, propulsion, and shift, this synergistic pair action is eccentric lengthening. This lengthening is storing elastic energy that will be released in the swing phase of the gait.
The lateral kinetic chain is in contralateral relationship with the anterior spiral kinetic chain: stance/swing. This movement requires stability across the anterior surface of the sacrum. The iliacus and contralateral piriformis become functional synergists during the swing phase of the gait. Looking at these kinds of contralateral relationships is an important aspect in movement assessment.
The iliacus and piriformis pictured here are in ipsilateral relationship. When the iliacus and piriformis are in contralateral relationship they create a functional X across the anterior surface of the sacrum.
Posterior Spiral ~ Generation of Stored Elastic Energy
The coiling of the thoracolumbar fascia acts on the sacrum and the SIJ. The hip is extending and externally rotating. The iliacus is actively engaged in eccentric lengthening, or is a functional opposite.
An up-regulated iliacus is going to down-regulate the coiling action of the posterior spiral kinetic chain. This is important when looking at the posterior surface muscles that act on the sacrum. Often, multifidus/sacrospinalis and gluteus maximus are down-regulated and need to get back into the equation for sacral stability.
Anterior Spiral ~ Translation of Stored Elastic energy
The iliacus is a powerful hip flexor. An up-regulated iliacus will look for recruits to assist in hip flexion during the swing phase of the gait. The common players the body looks to recruit are the psoas, tensor fasciae latea, rectus femoris, sartorius, and all the adductors.
The anterior spiral pairs with the contralateral lateral kinetic chain. At the moment when hip extension translates into hip flexion, the iliacus and the contralateral piriformis are in functional synergist relationship. This creates stability across the anterior sacrum during shock absorption.
Remote Relationships:
The body starts to look for recruitments to assist an up-regulated and fatigued muscle/s. One common recruitment pattern are muscles in contralateral pairs. The pectoralis minor and the iliacus are common up-regulated muscles, they work together in the contralateral shoulder to hip relationship of the anterior spiral.
Manual Therapy Application:
One important aspect of any manual intervention is to ask the body directly if the modality is appropriate. This can be verified by doing a little bit of release. Go back to the relationship and take notice. Did the response change in a favorable way? If it did, then the release technique was appropriate. If it did not, then the nervous system needs something else to restore the coordination.
Here are a few strategies I regularly employ when working with an up-regulated iliacus.
Strain Counter Strain:
This is a one of my favorite go to techniques. It is gentle and effective. There is little risk to further irritation of an up-regulated iliacus. The lessor trochanter, the common tendon junction and the bowl of the pelvis are good entry points for this gentle technique.
Belted Pelvis:
This active bilateral release can have a dramatic positive effect in the SIJ. The belt puts the SIJ in compression while the bilateral activation of internal/external rotation resets the receptors. The therapist can approach the release in two ways. One is to use feedback pressure to activate the balance between internal and external rotation. The other is to use bilateral pressure on both piriformi to reset the muscle spindles.
Active Muscle Spindle:
This is a technique that resets the muscle spindles interpretation of muscle length. Support clients leg with thigh vertical, leg horizontal. Have the client hold their leg in place to accurately access the common tendon junction near the bowl of the pelvis. The placement of the practitioners fingers should be such that there is zero visceral impingement. Once appropriate contact is made, the clientslowly extends the leg and draws back to the starting position.
Pin and Stretch:
This flossing technique is a mixed bag. It can either be highly effective or over stimulates the nervous system. Ask the body if it is appropriate to the client’s presentation.
Conclusion:
When assessing the players involved with sacral stability, ask if the identified players can cooperate with each other. Getting all the players back on the same team make for a happy sacrum.
Glossary:
Concentric activation ~ The muscle fibers are shortening; the muscle attachments are moving toward one another.
Eccentric activation ~ The muscle fibers are lengthening; the muscle attachments are moving away from one another.
Synergist ~ Muscles that work together during movement.
Functional Opposite ~ Muscles that work opposite to one another. One muscle is lengthening while the other is shortening.
Up-Regulated ~ An overstimulated muscle that is compensating for other muscle/s that are not participating. Often the muscle will become overworked and fatigued and unable to respond appropriately.
Down-Regulated ~ An under stimulated muscle. The function is impaired and unable to respond appropriately.
Reciprocal Inhibition ~ When a muscle/s is contracting, the opposite muscle/s must be lengthening. If the opposite muscle/s are unable to lengthen, being up-regulated for example, then that will functionally inhibit the muscle that is contracting.
*Please note this particular series of blogs will describe each of the four muscles and their relationship to the five principal actions described in the charts of The 5 Primary Kinetic Chain Poster Set I’ve developed. This is the first in a series of four posts. You can find the second post on the Iliacus here.
Introduction to the Sacrum:
The sacrum, or sacred bone, is unique in the body. Mystics regard the sacrum as the focal point for kundalini, the spiraling energy that rises from the root through the crown. This triangular shaped bone provides the base of support for the spinal column.
The sacrum articulates with the pelvis through the sacral iliac joint, SIJ. The kinetic energy of ground force reaction moves from the feet engaging the earth, up through the legs, into the pelvis. The energy crosses through the pelvis into the sacrum and up through the axis of the spine. The manner by which the energy moves into and through the axis of the spine defines our ability to respond to ground force reaction.
There are four important muscles that act directly on the sacrum.
Posterior Surface: multifidus/sacrospinalis & gluteus maximus
These four high level muscles often are not engaged with their task of stabilizing the sacrum through a spectrum of movement. When we look at the function of these four muscles, and the various movement they are involved in, there is a trend we see in most people’s presentation that are seeking therapeutic intervention.
The anterior surface muscles are often up-regulated. These muscles are over worked and do not respond appropriately. One of the flavors of synergistic dominance is when one group of fibers becomes up-regulated, those dominant fibers then down-regulate the function of that muscle over its spectrum of movement.
The posterior surface muscles are often down-regulated and are not available to respond appropriately to movement.
The relationship of how these four muscles work together in coordination changes over the spectrum of movement. The 5 Primary Kinetic Chains have unique principal actions that inform the sequence of movement. This series of essays will describe each of the four muscles and their relationship to the five Principal Actions I’ve described in the 5 Primary Kinetic Chains poster set.
Piriformis:
The piriformis is a flat, pyramidal shaped muscle that runs from the anterior surface of the sacrum to the greater trochanter of the femur. The manner by which the muscle fans across the broad surface of the sacrum is somewhat similar to the subscapularis attaching to the scapula. The piriformis is an external rotator of the femur; the subscapularis is an internal rotator of the humerus, thereby making them functional opposites.
Many people have challenges due to the structure and function of their piriformis. Approximately one in 5 of us have piriformis anomalies (Read more here). Those that have this are often grouped into a category of “piriformis syndrome,” a pattern of up-regulated piriformis that irritates and compresses the nerve bundles, the sciatica nerve, that pass through the muscle.
People that have this presentation are often challenged by common movement triggers. Prolonged sitting, driving, and — for some — simply walking, is enough to exacerbate the pressure of the muscle acting on the nerve.
Concentric Actions of The Piriformis:
Sagittal ~ hip extension & sacral flexion
Coronal ~ hip abduction & sacral downward/upward rotation (limited by SIJ gap)
Transverse ~ hip external rotation & sacral downward/upward rotation on an oblique axis
The Piriformis and The 5 Primary Kinetic Chains:
Intrinsic ~ Breath
The relationship between the piriformis and the pelvic floor is often a good starting point for evaluation. The following two scenarios are common presentations:
Spinal Wave:
The piriformis is a participant in the spinal wave during the breath cycle.
An up-regulated piriformis is the action of the exhalation phase thereby affecting the inhalation phase of the breath.
Pelvic Floor:
The sacral tuberous ligament, and the obturator internus help make up the extrinsic boundaries of the pelvic floor. The piriformis is a synergist to the obturator internus making it an easily recruitable option for an up-regulated pelvic floor.
Deep Longitudinal ~ Shock Absorption
An up-regulated piriformis interferes with the kinetic wave of shock absorption. The up-regulated piriformis is a bracing strategy for the SIJ. Compression in the SIJ functionally acts as an abutment to the kinetic wave of ground force reaction.
The body’s appropriate response to the kinetic wave of shock absorption is to counter with the push reflex. Imagine stepping off the curb. The hip must descend so that the foot can meet the ground. This is an eccentric action of the quadrates lumborum, the QL. An up-regulated piriformis down-regulates the push reflex.
The peroneal nerve, a division of the sciatic nerve, innervates the subsystem muscles of the deep longitudinal kinetic chain. An up-regulated piriformis that compresses the peroneal nerve will affect the peroneus muscles and the short head of the bicep femoris. When these subsystem muscles are unable to respond appropriately, the compensation is joint compression strategies that will move up the kinetic chain.
Lateral ~ Axial Stability
The gluteus medius, a lateral kinetic chain subsystem muscle, needs to play well with the piriformis. The piriformis is both a synergist and functional opposite to actions of the gluteus medius.
The gluteus medius attaches to the pelvis with a broad fan-like orientation of fibers. The action includes abduction of the hip, and internal and external rotation of the femur. This is significant because some fibers act as synergists and others act as functional opposites. Often, select fibers of an up-regulated gluteus medius will functionally down-regulate the other fibers. This contributes to an up-regulated piriformis.
The lateral kinetic chain is in contralateral relationship with the anterior spiral kinetic chain: stance / swing. This movement requires stability across the anterior surface of the sacrum. The contralateral iliacus and the piriformis become functional synergists during the swing phase of the gait.
The iliacus and piriformis pictured here are in ipsilateral relationship. When the iliacus and piriformis are in contralateral relationship they create a functional X across the anterior surface of the sacrum.
Posterior Spiral ~ Generation of Stored Elastic Energy
The coiling of the thoracolumbar fascia acts on the sacrum and the SIJ. The hip is extending and externally rotating. The piriformis is a synergist to the gluteus maximus, a posterior spiral subsystem muscle and sacral stabilizer.
Potentially any muscles in the posterior spiral kinetic chain could be in a synergistic dominance relationship.
Posterior spiral kinetic chain is paired with the contralateral deep longitudinal kinetic chain. The push leads the strike; the piriformi are in an alternating activation.
Anterior Spiral ~ Translation of Stored Elastic energy
The anterior spiral pairs with the contralateral lateral kinetic chain. At the moment when hip extension translates into hip flexion, the ipsilateral iliacus and the piriformis are in functional synergist relationship.
Remote Relationships:
The body starts to look for recruitments to assist an up-regulated and fatigued muscle. One common recruitment pattern is muscles that have similar fibril orientation. The lateral pterigoid is a common jaw remote relationship.
Manual Therapy Application:
One important aspect of any manual intervention is to ask the body directly if the modality is appropriate. This can be verified by doing a little bit of release. Go back to the relationship and take notice. Did the response change in a favorable way? If it did, then the release technique was appropriate. If it did not, then the nervous system needs something else to restore the coordination.
There are few strategies I regularly employ when working with an up-regulated piriformis.
Strain Counter Strain:
This is a one of my favorite go to techniques. It is gentle and effective. There is little risk to further irritation of an up-regulated piriformis.
Belted Pelvis:
This active bilateral release can have a dramatic positive effect in the SIJ. The belt puts the SIJ in compression while the bilateral activation of internal/external rotation resets the receptors. The therapist can approach the release in two ways. One is to use feedback pressure to activate the balance between internal and external rotation. The other is to use bilateral pressure on both piriformi to reset the muscle spindles.
Pin and Stretch:
This flossing technique is a mixed bag. It can either be highly effective or over stimulate the nervous system. Ask the body if it is appropriate to the client’s presentation.
Conclusion:
When assessing the players involved with sacral stability, ask if the players can cooperate with each other. Getting all the players back on the same team make for a happy sacrum.
Glossary:
Concentric activation ~ The muscle fibers are shortening; the muscle attachments are moving toward one another.
Eccentric activation ~ The muscle fibers are lengthening; the muscle attachments are moving away from one another.
Synergist ~ Muscles that work together during movement.
Functional Opposite ~ Muscles that work opposite to one another. One muscle is lengthening while the other is shortening.
Up-Regulated ~ An overstimulated muscle that is compensating for other muscle/s that are not participating. Often the muscle will become overworked and fatigued and unable to respond appropriately.
Down-Regulated ~ An under stimulated muscle. The function is impaired and unable to respond appropriately.
The stability or mobility question has been brought to the table many times. Which is more important ~ to be stable or to have mobility?
There are different perspectives to the answer depending on one’s field of study, the application, and the lens that you look through.
Here is my take: stability and mobility are in an interdependent relationship. One can’t effectively happen without the other.
Stability and mobility rely on each other to keep the structure safe. Stability is to software as mobility is to hardware. Stability requires motor control, the ability of the nervous system to respond appropriately as movement occurs. Mobility is the hardware, the organization of bones, joints, ligaments, tendons, muscles and fascial structures. The structure is responding to movement, messages of how movement is occurring, and how this information is being relayed up to the motor control center. A strategy is then derived as a response to the changing environment. The quality of movement being expressed is a product of integration of both stability and mobility.
Dynamic Stability is perhaps a better term to describe the product of stability and mobility. The question then shifts from “stability or mobility” to whether the body can appropriately respond to movement over a complete range of motion and a changing environment. For example, if you are hiking a steep loose trail, and the earth shifts under your feet, is the responsive mobility available for you to keep from losing footing and possibly spraining an ankle?
Dynamic Stability keeps the structure safe. The result of stability + mobility is neuromuscular integration that is available to respond appropriately to a complete range of motion. When life happens, and the environment shifts in an unforeseeable way, dynamic stability ensures an appropriate response is available.
In the movement known as the walking gait, the Lateral Kinetic Chain completes this dynamic platform. The body has just absorbed the kinetic energy through the deep longitudinal kinetic chain, the strike phase of the gait. That energy now needs to be grounded into a stable yet dynamic platform, the lateral kinetic chain, that will allow the body to generate the next movement, the power generation of the posterior spiral kinetic chain. The axis of the spine is integrating all three planes of motion while centralizing the energy from the previous shock absorption phase. As a result of dynamic stability, the body is prepared to generate propulsion, the forward motion of the walking gait.
The midline action of maintaining balance is another important action of the lateral kinetic chain. Complementary neuromuscular activations are working in cooperation to balance the relationship of movement, kinetic energy, gravity, and ground force reaction. These complementary actions provide the dynamic base so that the appendicular skeleton can generate energy.
Movement is a balancing act between environmental factors and the structure’s ability to respond appropriately. For example, when we look at the sculpture of rock stacking, we see the dance between the unique attributes of each rock. The size, shape, and center of gravity of each influences the balance point. Each rock complements the previous. The balance points create an axis, an axis of stability. Without this axis, the stack of stones would fall.
This demonstrates the third principal action of The 5 Primary Kinetic Chains ~ Axial Stability for Appendicular Mobility. When a dynamic base is in place, the appendicular skeleton can express its potential of generating stored elastic energy in movement.
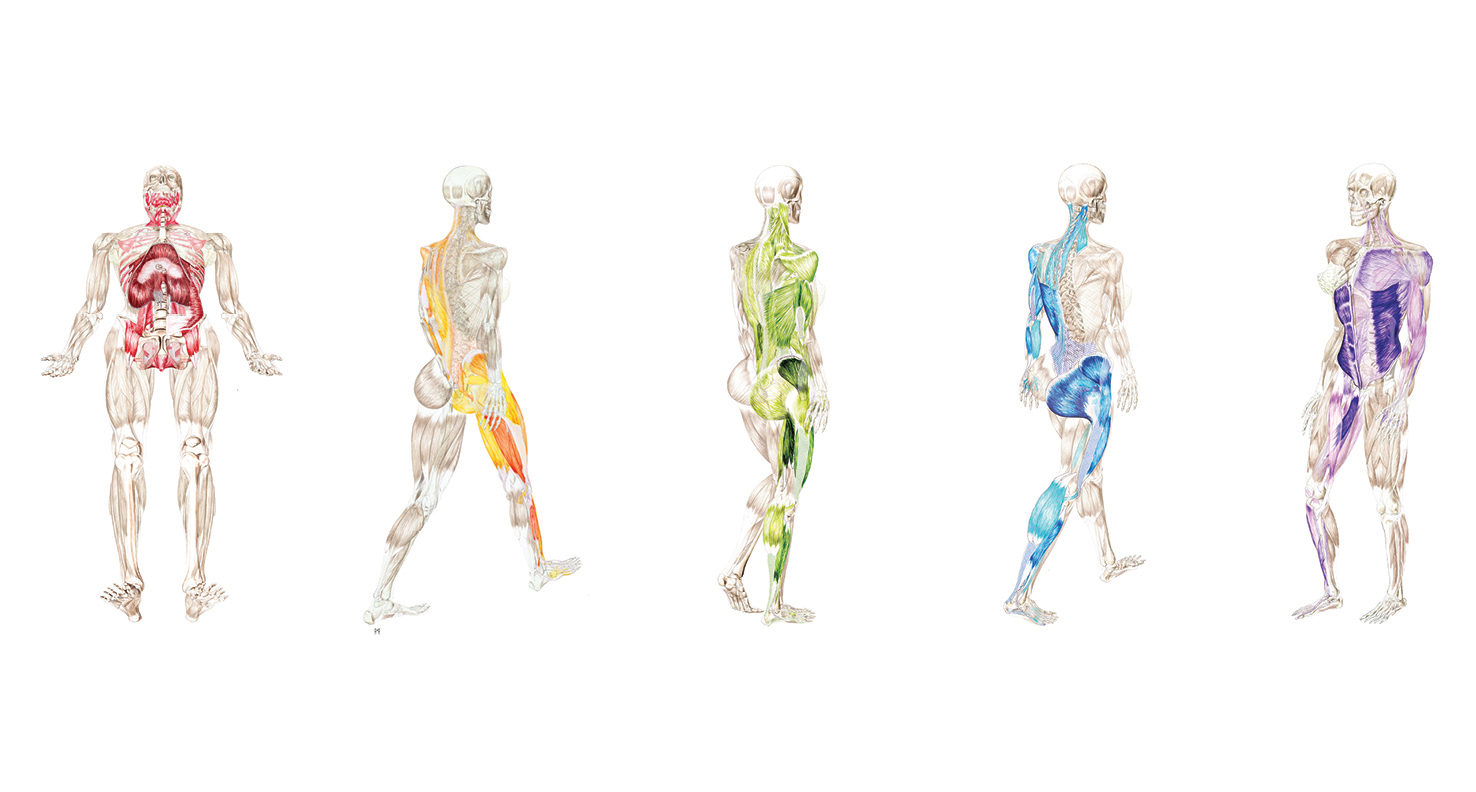
The 5 Primary Kinetic Chains are the master template for not only the walking gait as I’ve explored in my anatomy art, but for all locomotion and movement. Different movements have different relationships to gravity and the environment, and they use different muscular activations. (These activations are referred as kinetic chains, force transmission systems and sling systems.)
For example, swimming doesn’t have ground engagement like the strike phase of the gait. Instead, the spear phase (reaching through the water) is analogous to the deep longitudinal system. The kinetic sequence runs from the hand and through the anterior body to the opposite leg. The arm lines are doing the work in swimming that the leg lines are doing in walking.
Let’s dissect The 5 Primary Kinetic Chains as movement concepts:
1) Intrinsic:
The intrinsic system is the nervous system’s relationship to breathing. Our breathing apparatus, the mechanism of pressurization systems, has a direct effect on the autonomic nervous system. “You can’t own your movement until you own your breath.” This is about our breath mastery in relationship to our movement.
2) Deep Longitudinal:
The deep longitudinal system is about shock absorption. Shock absorption is the ability for kinetic energy to wave through the body joint by joint. If the wave is unable to move freely through the fascial system, that energy has to be absorbed in some way (such as a compensation). Imagine ocean waves breaking on the beach. The forces flow rhythmically absorbed by the sand. Now put a rocky buttress in front of the same wave and there is a tumultuous energy exchange of the crashing into the buttress.
3) Lateral:
The lateral system is the midline stability of the structure. The axis of the spine (axial skeleton) needs dynamic stability so that the appendicular skeleton has a platform by which to generate energy. Without the stability of the axis, the arms and legs will be impaired to generate power or work production.
4) Posterior Spiral:
The posterior spiral is the generation of stored elastic energy. The fascial matrix is a potential energy system. Efficient movement uses muscular activation to act on the fascial system. The fascial system spreads the load over as much area as possible which increases efficiency. As the energy winds up in the tissues, the potential release of that energy assists work production in the complementary movement.
5) Anterior Spiral:
The anterior spiral is the release of elastic energy into the complementary movement. Elastic energy can be released in different ways across the structure. When you are watching graceful athletes moving in profound ways, you are seeing elastic energy being stored and released in an efficient way. The energy is spread across the entire fascial fabric and the result is seemingly effortless movement.
These concepts are always present in integrated movement:
Breath~Shock Absorption~Axial Stability~Stored Elastic Energy~Translation of Elastic Energy