Please note this particular series of blogs will describe each of the four muscles and their relationship to the five principal actions described in the charts of The 5 Primary Kinetic Chain Poster Set I’ve developed. This is Part Two of four. You can find Part One on the Piriformis here.
Introduction:
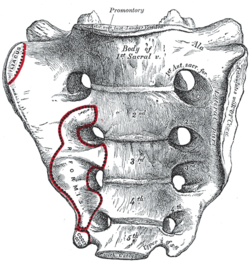
The sacrum, or sacred bone, is unique in the body. Mystics regard the sacrum as the focal point for kundalini, the spiraling energy that rises from the root through the crown. This triangular shaped bone provides the base of support for the spinal column.
The sacrum articulates with the pelvis through the sacral iliac joint, SIJ. The kinetic energy of ground force reaction moves from the feet engaging the earth, up through the legs, into the pelvis. The energy crosses through the pelvis into the sacrum and up through the axis of the spine. The manner by which this energy moves into and through the axis of the spine defines our ability to respond to ground force reaction.
There are four important muscles that act directly on the sacrum.
Anterior Surface:
iliacus
Posterior Surface:
multifidus/sacrospinalis
gluteus maximus
These four high level muscles often are not engaged with their task of stabilizing the sacrum through a spectrum of movement. When we look at the function of these four muscles, and the various movement they are involved in, there is a trend we see in most people’s presentation that are seeking therapeutic intervention.
The anterior surface muscles are often up-regulated. These muscles are over worked and do not respond appropriately. One of the flavors of synergistic dominance is when one group of fibers becomes up-regulated, those dominant fibers then down-regulate the function of that muscle over its spectrum of movement.
The posterior surface muscles are often down-regulated and are not available to respond appropriately to movement.
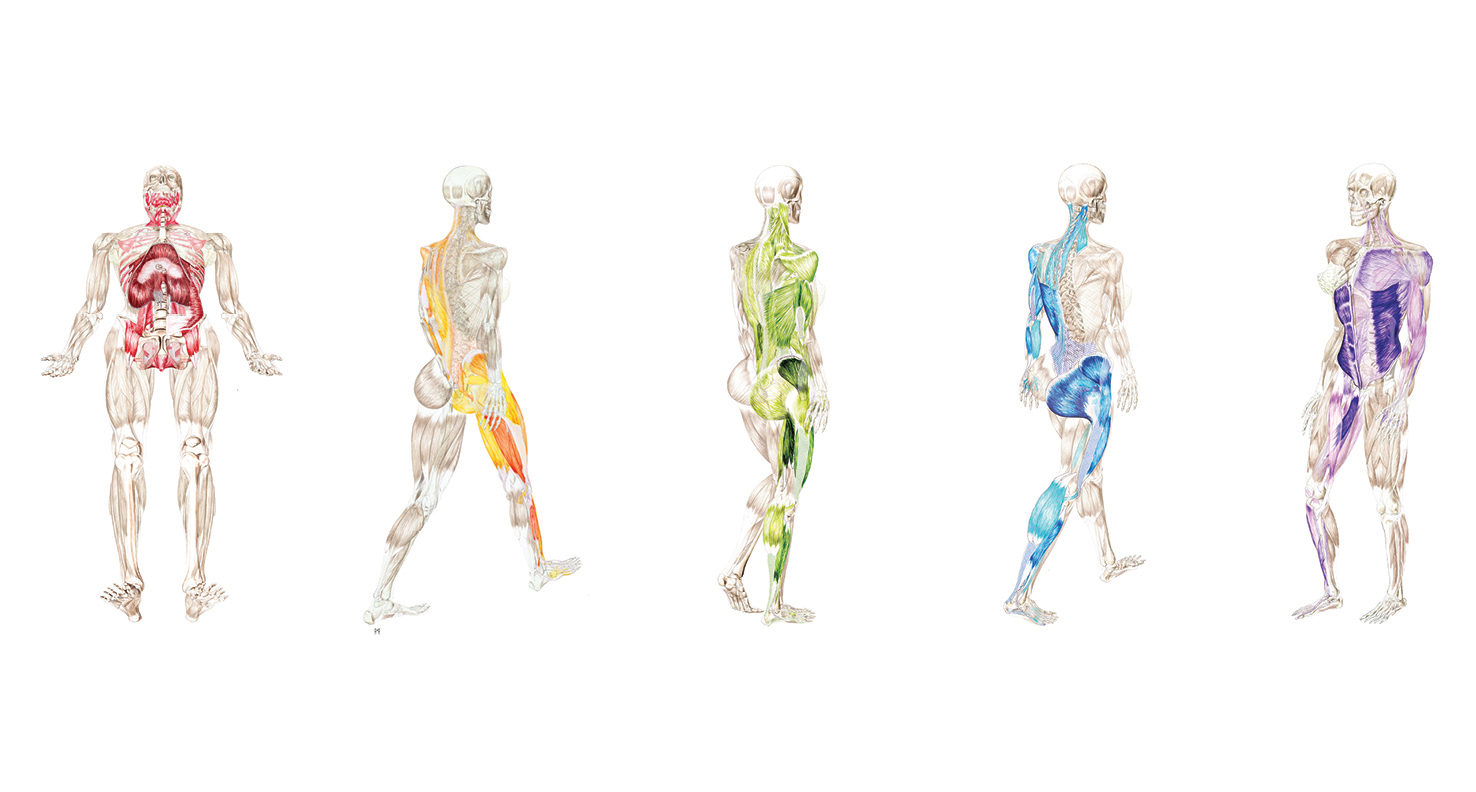
The relationship of how these four muscles work together in coordination changes over the spectrum of movement. The 5 Primary Kinetic Chains have unique Principal Actions that inform the sequence of movement. This series of essays will describe each of the four muscles and their relationship to the five principal actions.
Ilacus:
The iliacus is a large primary muscle of the pelvis that attaches to the bowl of the pelvis, the iliac fossa. This muscle has a large surface area as it fans across the inner bowl of the pelvis. The multiple direction of these fibers give them advantage over a range of functions.
As the fibers of the iliacus come off the pelvic bowl, they knit together multiple structures of the pelvis. Fibers attach to the anterior sacral ligaments, the sacrum, the psoas, and the lessor trochantor of the femur.
Looking at the web of connective tissue between the iliacus, the psoas, the anterior sacral ligaments, and the direct attachment on the body of the sacrum, it becomes clear that the iliacus has a profound effect on the sacrum.
The fibers of the iliacus are joined by the fibers of the psoas. Together they create a common tendon attachment on the lesser trochanter. This makes the iliacus and the psoas an important synergistic pair, yet they have some different roles in movement.
The psoas is a multi-segmented muscle. The psoas crosses multiple joints of the lumbar spine. Muscles that cross multiple joints have an important role as a stabilizer during the work production phase of movement. The shorter fibered muscles that cross one joint are the hard working prime mover. The important distinction here is that the psoas is acting on the lumbar spine while the iliacus is acting on the pelvis. When these two muscles are not playing well as individuals, or as a synergistic pair, the result is a destabilized lumbar-pelvis.
The iliacus is considered one of the more common up-regulated muscles. The bracing, or shortening action of an up-regulated iliacus, affects the sacroiliac joint, SIJ.
As the iliacus acts on the ilium, the relationship of a neutral SIJ becomes altered. The movement of the sacrum is self-limiting by the SIJ, while the ilium has more freedom to move around the sacrum creating a mobile/stable relationship. Hip rotation, hip hiking, and hip flare are relationships to sagittal, coronal, and transverse plane movement. The iliacus is involved in these movements even if it isn’t the driver.
Concentric Actions of The Iliacus:
Sagittal ~ hip flexion, ilium rotation, & sacral flexion
Coronal ~ hip adduction, ilium elevation & sacral downward/upward rotation (self-limiting)
Transverse ~ hip external rotation, ilium flare & sacral downward/upward rotation on an oblique axis
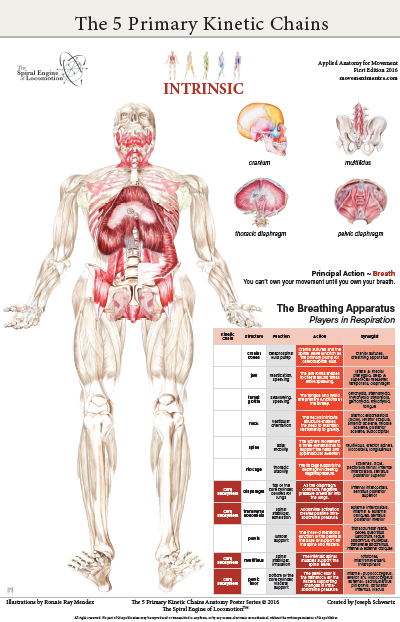
The Iliacus and The 5 Primary Kinetic Chains:
Intrinsic ~ Breath
The iliacus is considered an extrinsic muscle of the pelvic floor. When you consider movement of the ilium, sacrum, and hip, the pelvic floor is involved.
The following two scenarios are common presentations:
Spinal Wave:
The iliacus is a participant in the spinal wave during the breath cycle.
Inhalation Phase: pelvic floor/eccentric action ~ spine/extension action
Exhalation Phase: pelvic floor/concentric action ~ spine/flexion action
An up-regulated iliacus is the action of the exhalation phase thereby affecting the inhalation phase of the breath. This is a relationship of reciprocal inhibition.
Pelvic Floor:
The iliacus attaches on the bowl of the pelvis creating an extrinsic boundary. An up-regulated iliacus partners with the pelvic floor. During the inhalation phase of the breath, the pelvic floor’s action is eccentric lengthening. An up-regulated pelvic floor loses this ability.
Deep Longitudinal ~ Shock Absorption
An up-regulated iliacus interferes with the kinetic wave of shock absorption. The up-regulated iliacus is a bracing strategy for the SIJ. Compression in the SIJ functionally acts as an abutment to the kinetic wave of ground force reaction.
The body’s appropriate response to the kinetic wave of shock absorption is to counter with the push reflex. Imagine stepping off the curb. The hip must descend so that the foot can meet the ground. This is an eccentric action of the quadrates lumborum, the QL. An up-regulated iliacus down-regulates the push reflex.
Lateral ~ Axial Stability
The adductor magnus, a lateral kinetic chain subsystem muscle, needs to play well with the iliacus. The adductor magnus is a synergist with the adductor longus. The iliacus is synergist with the adductor longus.
During the transition phases of the gait, mid stance, late stance, propulsion, and shift, this synergistic pair action is eccentric lengthening. This lengthening is storing elastic energy that will be released in the swing phase of the gait.
The lateral kinetic chain is in contralateral relationship with the anterior spiral kinetic chain: stance/swing. This movement requires stability across the anterior surface of the sacrum. The iliacus and contralateral piriformis become functional synergists during the swing phase of the gait. Looking at these kinds of contralateral relationships is an important aspect in movement assessment.
Posterior Spiral ~ Generation of Stored Elastic Energy
The coiling of the thoracolumbar fascia acts on the sacrum and the SIJ. The hip is extending and externally rotating. The iliacus is actively engaged in eccentric lengthening, or is a functional opposite.
An up-regulated iliacus is going to down-regulate the coiling action of the posterior spiral kinetic chain. This is important when looking at the posterior surface muscles that act on the sacrum. Often, multifidus/sacrospinalis and gluteus maximus are down-regulated and need to get back into the equation for sacral stability.
Anterior Spiral ~ Translation of Stored Elastic energy
The iliacus is a powerful hip flexor. An up-regulated iliacus will look for recruits to assist in hip flexion during the swing phase of the gait. The common players the body looks to recruit are the psoas, tensor fasciae latea, rectus femoris, sartorius, and all the adductors.
The anterior spiral pairs with the contralateral lateral kinetic chain. At the moment when hip extension translates into hip flexion, the iliacus and the contralateral piriformis are in functional synergist relationship. This creates stability across the anterior sacrum during shock absorption.
Remote Relationships:
The body starts to look for recruitments to assist an up-regulated and fatigued muscle/s. One common recruitment pattern are muscles in contralateral pairs. The pectoralis minor and the iliacus are common up-regulated muscles, they work together in the contralateral shoulder to hip relationship of the anterior spiral.
Manual Therapy Application:
One important aspect of any manual intervention is to ask the body directly if the modality is appropriate. This can be verified by doing a little bit of release. Go back to the relationship and take notice. Did the response change in a favorable way? If it did, then the release technique was appropriate. If it did not, then the nervous system needs something else to restore the coordination.
Here are a few strategies I regularly employ when working with an up-regulated iliacus.
Strain Counter Strain:
This is a one of my favorite go to techniques. It is gentle and effective. There is little risk to further irritation of an up-regulated iliacus. The lessor trochanter, the common tendon junction and the bowl of the pelvis are good entry points for this gentle technique.
Belted Pelvis:
This active bilateral release can have a dramatic positive effect in the SIJ. The belt puts the SIJ in compression while the bilateral activation of internal/external rotation resets the receptors. The therapist can approach the release in two ways. One is to use feedback pressure to activate the balance between internal and external rotation. The other is to use bilateral pressure on both piriformi to reset the muscle spindles.
Active Muscle Spindle:
This is a technique that resets the muscle spindles interpretation of muscle length. Support clients leg with thigh vertical, leg horizontal. Have the client hold their leg in place to accurately access the common tendon junction near the bowl of the pelvis. The placement of the practitioners fingers should be such that there is zero visceral impingement. Once appropriate contact is made, the client slowly extends the leg and draws back to the starting position.
Pin and Stretch:
This flossing technique is a mixed bag. It can either be highly effective or over stimulates the nervous system. Ask the body if it is appropriate to the client’s presentation.
Conclusion:
When assessing the players involved with sacral stability, ask if the identified players can cooperate with each other. Getting all the players back on the same team make for a happy sacrum.
Glossary:
Concentric activation ~ The muscle fibers are shortening; the muscle attachments are moving toward one another.
Eccentric activation ~ The muscle fibers are lengthening; the muscle attachments are moving away from one another.
Synergist ~ Muscles that work together during movement.
Functional Opposite ~ Muscles that work opposite to one another. One muscle is lengthening while the other is shortening.
Up-Regulated ~ An overstimulated muscle that is compensating for other muscle/s that are not participating. Often the muscle will become overworked and fatigued and unable to respond appropriately.
Down-Regulated ~ An under stimulated muscle. The function is impaired and unable to respond appropriately.
Reciprocal Inhibition ~ When a muscle/s is contracting, the opposite muscle/s must be lengthening. If the opposite muscle/s are unable to lengthen, being up-regulated for example, then that will functionally inhibit the muscle that is contracting.