I’d like to talk with you about an anecdotal experience I recently had with a client.
I had a runner come to me who was experiencing knee pain. If I had stopped in my assessment at simply looking at the function of the knee, I would have missed the primary driver of the compensation pattern. Because I linked the relationship of the Anterior Kinetic Chain, and the core cylinder, I was able to correlate an internal oblique issue to the medial knee. It’s not uncommon for ligaments to compensate for the burden when muscular function is impaired. My ability to move beyond the obvious to a deeper level of inquiry – which is what we learn in Dynamic Neuromuscular Assessment™ Seminars – allowed me to get to the more profound root issue for my client.
Anatomy and kinesiology are two disciplines that give clarity to the interdependence of the structure and movement of the body.
Anatomy is the language used to describe the parts. These parts then fit together into systems that synergistically make up the whole organism.
Kinesiology is the language of movement. Through kinesiology, anatomy is given a context. If the language of movement is a symphony, the role of anatomy is to describe the source of each note of music.
Anatomy charts provide the fundamental foundation for understanding the names of bones, joints, ligaments, tendons, muscles, fascia, and so forth – the structure. Kinesiology then defines how each aspect of structure works together to create movement.
One of my teachers, early on in my career, imparted the importance of the breath, movement, and structure as being interdependent.
Movement is a translator to how the structure organizes, movement can’t lie. When the body is experiencing pain, the brain reorganizes movement so that we move around our pain instead of through it. This avoidance is a compensation to keep us in a perceived safe zone. As practitioners, our ability to see deviation in movement is paramount to assisting our clients. Often the walking gait is the lens through which we look during assessment. The 5 Primary Kinetic Chains provide a map of the gait.
The use of color in The 5 Primary Kinetic Chains illustrations imparts upon the teacher/student or practitioner/client, how the body organizes during movement. The kinetic chain charts further define how the body organizes in the optimal manner during gait. Why the gait? The gait is universal to human movement. From birth, our nervous system is prewired for developmental movement with the intention to get us upright and biped. If you have interest in a more in-depth conversation on the walking gait, see my blog on the Master Template. The synergistic organization, or sequential muscular activation, gives context to efficient movement and helps us to identify potential dysfunctional relationships that may not be obvious at first impression to the client or practitioner.
When the synergistic organization of our movement becomes less than optimal, or compensated, the result are over and underworked players. Synergistic dominance is the relationship between these over and under worked players. As a practitioner it is useful to have reference tools – like The 5 Primary Kinetic Chains Poster Set or Desktop Edition to help us dig deeper into the function and dysfunction presented by our clients.
Please leave a comment below about a powerful experience you had either as a client or practitioner where you or they went beyond the obvious to the profound!
Muscles produce work in the body. They come in two distinct types, smooth and striated. Smooth muscles are governed by the autonomic nervous system. Their function is automatic. Smooth muscles perform the regulatory functions. The tissues that make up organs, the GI tract, and arteries utilize smooth muscles to perform their unique functions. Conversely, striated muscles are governed by the rules of conscious motor control. Striated muscles are often referred to as skeletal muscles. Their job is to act on the skeleton for posture and movement.
Skeletal muscles have a spectrum of roles. Highlights include: work production, multiple joint stabilization, and position sense. Muscles need to be available to do their job in the movement equation. If they can’t participate appropriately, the brain will come up with a coping strategy. This is a survival-based mechanism, and this is what we call compensation. Compensation has many flavors, and despite a bad rap, it is the intelligence of the body doing its best to keep you safe.
Muscles come in many configurations. Generally, the large powerhouse muscles are more superficial, while the intrinsic stabilizers are deeper. Some muscles are specific in fibril orientation and function while others are available for multiple roles. For example, the large powerhouse muscles of the posterior chain, the latissimus dorsi and gluteus maximus, have multiple fibril orientations that look like a fan. This gives these muscles mechanical advantage over the range-of-motion spectrum.
For simplicity, let’s categorize muscles into two sets: short and long-lever. Short-lever muscles are the dependable hardworking muscles. They have mechanical advantage on the joint. The brain likes to use them as the go-to muscle during work production. Long-lever muscles cross multiple joints and have multiple attachments. Long-lever muscles are best suited for stabilization during work production. Their role is key when movement deviates and unknown variables occur in the environment.
Compensation patterns have a common trait among short and long-lever muscles: short-lever muscles are the heroes. They come to rescue when the long-lever muscles are not responding appropriately in the movement environment.
Short-Lever Muscles:
– cross one joint
– mechanical advantage
– commonly up-regulated
Long-Lever Muscles:
– cross multiple joints
– stabilizer during work production
– commonly down-regulated
Common Relationships:
Short-Lever ~ Long-Lever
Tibia Rotation
popliteus ~ bíceps femoris
Knee Flexion
bíceps femoris short head ~ biceps femoris long head
Hip Flexion
iliacus ~ psoas
Spinal Extension
multifidus ~ erector spinea
Shoulder Abduction
subclavius ~ pectoralis major
Elbow Flexion
brachialis ~ biceps brachii
These examples are samples of utilizing short-lever ~ long-lever muscle relationships to assess movement compensation patterns. The kinetic chain charts in The 5 Primary Kinetic Chains provide a map for investigating synergistic dominance, regional interdependence, and functional opposite musculoskeletal relationships. Muscles are in constant response to joint position in the movement environment. Can the muscles in conjunction with motor control instructions respond appropriately to the environment?
My upcoming Dynamic Neuromuscular Assessment™ workshops (learn more here) will provide an integrated strategy for movement assessment in a changing environment. Some of the key skill-sets we will employ:
utilizing a hybrid that combines direct assessment with indicator testing to uncover functional dysfunctional movement
utilizing feed-forward motor control to assess structure that cannot be directly tested
completing the proprioceptive feedback loop to assess both motor instructions and structural response
investigating long series kinetic chains because muscles do not work in isolation, they work in synergistic sequences during movement
investigating dynamic stability as a two-part equation: concentric action balanced by eccentric action — eccentric movement evaluation uncovers hidden layers of compensation
Please note this particular series of blogs will describe each of the four muscles and their relationship to the five principal actions described in the charts of The 5 Primary Kinetic Chain Poster Set I’ve developed. This is Part Two of four. You can find Part One on the Piriformis here.
Introduction:
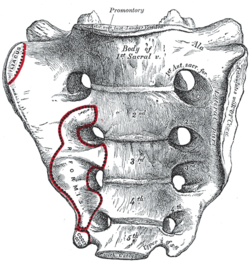
The sacrum, or sacred bone, is unique in the body. Mystics regard the sacrum as the focal point for kundalini, the spiraling energy that rises from the root through the crown. This triangular shaped bone provides the base of support for the spinal column.
The sacrum articulates with the pelvis through the sacral iliac joint, SIJ. The kinetic energy of ground force reaction moves from the feet engaging the earth, up through the legs, into the pelvis. The energy crosses through the pelvis into the sacrum and up through the axis of the spine. The manner by which this energy moves into and through the axis of the spine defines our ability to respond to ground force reaction.
There are four important muscles that act directly on the sacrum.
Posterior Surface:
multifidus/sacrospinalis
gluteus maximus
These four high level muscles often are not engaged with their task of stabilizing the sacrum through a spectrum of movement. When we look at the function of these four muscles, and the various movement they are involved in, there is a trend we see in most people’s presentation that are seeking therapeutic intervention.
The anterior surface muscles are often up-regulated. These muscles are over worked and do not respond appropriately. One of the flavors of synergistic dominance is when one group of fibers becomes up-regulated, those dominant fibers then down-regulate the function of that muscle over its spectrum of movement.
The posterior surface muscles are often down-regulated and are not available to respond appropriately to movement.
The relationship of how these four muscles work together in coordination changes over the spectrum of movement. The 5 Primary Kinetic Chains have unique Principal Actions that inform the sequence of movement. This series of essays will describe each of the four muscles and their relationship to the five principal actions.
Ilacus:
The iliacus is a large primary muscle of the pelvis that attaches to the bowl of the pelvis, the iliac fossa. This muscle has a large surface area as it fans across the inner bowl of the pelvis. The multiple direction of these fibers give them advantage over a range of functions.
As the fibers of the iliacus come off the pelvic bowl, they knit together multiple structures of the pelvis. Fibers attach to the anterior sacral ligaments, the sacrum, the psoas, and the lessor trochantor of the femur.
Looking at the web of connective tissue between the iliacus, the psoas, the anterior sacral ligaments, and the direct attachment on the body of the sacrum, it becomes clear that the iliacus has a profound effect on the sacrum.
The fibers of the iliacus are joined by the fibers of the psoas. Together they create a common tendon attachment on the lesser trochanter. This makes the iliacus and the psoas an important synergistic pair, yet they have some different roles in movement.
The psoas is a multi-segmented muscle. The psoas crosses multiple joints of the lumbar spine. Muscles that cross multiple joints have an important role as a stabilizer during the work production phase of movement. The shorter fibered muscles that cross one joint are the hard working prime mover. The important distinction here is that the psoas is acting on the lumbar spine while the iliacus is acting on the pelvis. When these two muscles are not playing well as individuals, or as a synergistic pair, the result is a destabilized lumbar-pelvis.
The iliacus is considered one of the more common up-regulated muscles. The bracing, or shortening action of an up-regulated iliacus, affects the sacroiliac joint, SIJ.
As the iliacus acts on the ilium, the relationship of a neutral SIJ becomes altered. The movement of the sacrum is self-limiting by the SIJ, while the ilium has more freedom to move around the sacrum creating a mobile/stable relationship. Hip rotation, hip hiking, and hip flare are relationships to sagittal, coronal, and transverse plane movement. The iliacus is involved in these movements even if it isn’t the driver.
Concentric Actions of The Iliacus:
Sagittal ~ hip flexion, ilium rotation, & sacral flexion
Transverse ~ hip external rotation, ilium flare & sacral downward/upward rotation on an oblique axis
The Iliacus and The 5 Primary Kinetic Chains:
Intrinsic ~ Breath
The iliacus is considered an extrinsic muscle of the pelvic floor. When you consider movement of the ilium, sacrum, and hip, the pelvic floor is involved.
The following two scenarios are common presentations:
Spinal Wave:
The iliacus is a participant in the spinal wave during the breath cycle.
An up-regulated iliacus is the action of the exhalation phase thereby affecting the inhalation phase of the breath. This is a relationship of reciprocal inhibition.
Pelvic Floor:
The iliacus attaches on the bowl of the pelvis creating an extrinsic boundary. An up-regulated iliacus partners with the pelvic floor. During the inhalation phase of the breath, the pelvic floor’s action is eccentric lengthening. An up-regulated pelvic floor loses this ability.
Deep Longitudinal ~ Shock Absorption
An up-regulated iliacus interferes with the kinetic wave of shock absorption. The up-regulated iliacus is a bracing strategy for the SIJ. Compression in the SIJ functionally acts as an abutment to the kinetic wave of ground force reaction.
The body’s appropriate response to the kinetic wave of shock absorption is to counter with the push reflex. Imagine stepping off the curb. The hip must descend so that the foot can meet the ground. This is an eccentric action of the quadrates lumborum, the QL. An up-regulated iliacus down-regulates the push reflex.
Lateral ~ Axial Stability
The adductor magnus, a lateral kinetic chain subsystem muscle, needs to play well with the iliacus. The adductor magnus is a synergist with the adductor longus. The iliacus is synergist with the adductor longus.
During the transition phases of the gait, mid stance, late stance, propulsion, and shift, this synergistic pair action is eccentric lengthening. This lengthening is storing elastic energy that will be released in the swing phase of the gait.
The lateral kinetic chain is in contralateral relationship with the anterior spiral kinetic chain: stance/swing. This movement requires stability across the anterior surface of the sacrum. The iliacus and contralateral piriformis become functional synergists during the swing phase of the gait. Looking at these kinds of contralateral relationships is an important aspect in movement assessment.
The iliacus and piriformis pictured here are in ipsilateral relationship. When the iliacus and piriformis are in contralateral relationship they create a functional X across the anterior surface of the sacrum.
Posterior Spiral ~ Generation of Stored Elastic Energy
The coiling of the thoracolumbar fascia acts on the sacrum and the SIJ. The hip is extending and externally rotating. The iliacus is actively engaged in eccentric lengthening, or is a functional opposite.
An up-regulated iliacus is going to down-regulate the coiling action of the posterior spiral kinetic chain. This is important when looking at the posterior surface muscles that act on the sacrum. Often, multifidus/sacrospinalis and gluteus maximus are down-regulated and need to get back into the equation for sacral stability.
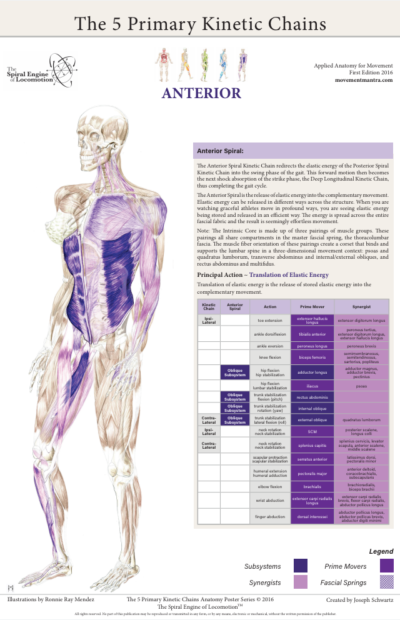
Anterior Spiral ~ Translation of Stored Elastic energy
The iliacus is a powerful hip flexor. An up-regulated iliacus will look for recruits to assist in hip flexion during the swing phase of the gait. The common players the body looks to recruit are the psoas, tensor fasciae latea, rectus femoris, sartorius, and all the adductors.
The anterior spiral pairs with the contralateral lateral kinetic chain. At the moment when hip extension translates into hip flexion, the iliacus and the contralateral piriformis are in functional synergist relationship. This creates stability across the anterior sacrum during shock absorption.
Remote Relationships:
The body starts to look for recruitments to assist an up-regulated and fatigued muscle/s. One common recruitment pattern are muscles in contralateral pairs. The pectoralis minor and the iliacus are common up-regulated muscles, they work together in the contralateral shoulder to hip relationship of the anterior spiral.
Manual Therapy Application:
One important aspect of any manual intervention is to ask the body directly if the modality is appropriate. This can be verified by doing a little bit of release. Go back to the relationship and take notice. Did the response change in a favorable way? If it did, then the release technique was appropriate. If it did not, then the nervous system needs something else to restore the coordination.
Here are a few strategies I regularly employ when working with an up-regulated iliacus.
Strain Counter Strain:
This is a one of my favorite go to techniques. It is gentle and effective. There is little risk to further irritation of an up-regulated iliacus. The lessor trochanter, the common tendon junction and the bowl of the pelvis are good entry points for this gentle technique.
Belted Pelvis:
This active bilateral release can have a dramatic positive effect in the SIJ. The belt puts the SIJ in compression while the bilateral activation of internal/external rotation resets the receptors. The therapist can approach the release in two ways. One is to use feedback pressure to activate the balance between internal and external rotation. The other is to use bilateral pressure on both piriformi to reset the muscle spindles.
Active Muscle Spindle:
This is a technique that resets the muscle spindles interpretation of muscle length. Support clients leg with thigh vertical, leg horizontal. Have the client hold their leg in place to accurately access the common tendon junction near the bowl of the pelvis. The placement of the practitioners fingers should be such that there is zero visceral impingement. Once appropriate contact is made, the clientslowly extends the leg and draws back to the starting position.
Pin and Stretch:
This flossing technique is a mixed bag. It can either be highly effective or over stimulates the nervous system. Ask the body if it is appropriate to the client’s presentation.
Conclusion:
When assessing the players involved with sacral stability, ask if the identified players can cooperate with each other. Getting all the players back on the same team make for a happy sacrum.
Glossary:
Concentric activation ~ The muscle fibers are shortening; the muscle attachments are moving toward one another.
Eccentric activation ~ The muscle fibers are lengthening; the muscle attachments are moving away from one another.
Synergist ~ Muscles that work together during movement.
Functional Opposite ~ Muscles that work opposite to one another. One muscle is lengthening while the other is shortening.
Up-Regulated ~ An overstimulated muscle that is compensating for other muscle/s that are not participating. Often the muscle will become overworked and fatigued and unable to respond appropriately.
Down-Regulated ~ An under stimulated muscle. The function is impaired and unable to respond appropriately.
Reciprocal Inhibition ~ When a muscle/s is contracting, the opposite muscle/s must be lengthening. If the opposite muscle/s are unable to lengthen, being up-regulated for example, then that will functionally inhibit the muscle that is contracting.
The charts in the Five Primary Kinetic Chains Anatomy Poster Series outline a primary physiological principle in movement: bones, joints, ligaments, tendons, muscles and fascia do not work in isolation. They work synergistically to create movement.
When movement is balanced and efficient, the players are all cooperating with each other. If movement is out of balance and inefficient, the result is compensation in the structure. This maladaptive compensation follows some specific physiological principles.
The first of these principles, synergistic dominance, is when one synergistic component of the structure is compensating for another synergistic component. More specifically, one component is overworked or up-regulated in relationship with another synergist that is underworked or down-regulated.
Synergistic dominance can show up over a spectrum of compensatory strategies. It can show up locally or globally. A local example would be the relationship of a muscle to itself. The distal end of a muscle can be up-regulated for a down-regulated proximal end of the same muscle. Synergist dominance will also show up when multiple muscles are working together. For example, hip flexion has several muscles that work synergistically. The iliacus, psoas, tensor fasciae latea, rectus femoris, adductor longus, and sartorious are the major contributors to hip flexion. If one of these muscles is up-regulated, that can functionally down-regulate the others.
Synergistic dominance also shows up globally. Kinetic chains, the manner in which the musculoskeletal system organizes itself, is not merely a local occurrence. Kinetic chains organize across the entire fascial fabric. The lateral kinetic chain provides a good example of global synergistic dominance. Throughout the dynamic platform of the stance phase of the gait, the ankle, pelvis, torso, and neck all need to play well together. If they are unable to do so, then one player will take over doing the job of the player unable to engage. Single leg stance is a great global assessment protocol to discern synergistic dominance of the lateral kinetic chain.
Synergistic dominance can also show up in kinetic chains that work in unison. For example, during the gait cycle, the posterior spiral kinetic chain is paired with the opposite deep longitudinal kinetic chain. Likewise, the lateral kinetic chain is paired with the opposite anterior spiral kinetic chain. These pairings of kinetic chains have an interdependent relationship. One relies on the other in the efficiency of storing and releasing elastic energy. If one chain has a dysfunctional component, it is going to have an effect on the other, they are in a synergistic relationship.
The other side of the synergist coin is the functional opposite. Muscles that work in opposition to one another rely on a principal called reciprocal inhibition. Reciprocal inhibition defines that the agonist, contracts or shortens, as the opposite, the antagonist, must lengthen. Simply, if one muscle is shortening then the other must be lengthening. If the muscle that should be lengthening is unable to do so, the effect is that the muscle that needs to shorten becomes down-regulated. It is unable to overcome the up-regulated muscle, as it can’t compete.
Functional opposites happen across kinetic chains just as synergists do. The foundation of understanding synergistic dominance builds the prerequisite for investigating functional opposites. As movement evolves, essentially there are two things happening: some tissues are shortening while others are lengthening.
The charts included in The 5 Primary Kinetic Chains posters provide a map for synergistic relationships. By mapping the synergists, one can then decode functional opposites. This is a very useful learning tool as well as a visual reference for your clients and patients.