Bodies by both function and design require movement. Generally speaking, our movement requirements as humans have evolved and devolved due to societal constraints. We no longer receive our daily requirement of movement as hunters and gatherers surviving in our environment. Because our environment has changed, the way we embody exercise and our daily requirement of movement must also change.
Our bodies require attention to perform optimally. For example, we need to provide the right fuel through food that feeds and supports our bodies. Eating the wrong foods leads to poor health and our vitality diminishes. The same is true with movement. If we don’t move well, our health and vitality diminishes. We experience this through discomfort, pain, and/or injury.
The good news is that we can utilize the quality of our movement as preventive maintenance. There is great wisdom in the saying: “an ounce of prevention is worth a pound of cure.” My go to preventative medicine is joint flossing. Joint flossing is the oscillation of movement across the joint and it is the preventive maintenance that your body craves. Joint flossing is the foundation that all your other movement activities build off of. Joint flossing is at the heart and soul of my personal practice.
Knowing that skills are developed over time, rarely can we jump into something new and be proficient. The nuance of activity takes time to develop. In movement, joint flossing is the developmental work our bodies and brain crave. However, because our mind is easily bored and is always looking for the next new and shiny adventure, it takes attention and discipline to develop a solid foundation. In martial arts they say: to master one thing leads to mastering many. With movement, this begins with joint flossing.
Skills development is a progression. One skill builds on the next. The movement programs I’ve developed in Dynamic Neuromuscular Assessment honor this progression. In each program, the movement skills are delivered incrementally so that your nervous system can respond sustainably. Whether you choose to dip your toe in the water and start with the Fabulous Feet program or take the deep dive with the Gait Master Course, after a few months of consistent daily practice, you body will reward your mind with the health and vitality that comes from recovering movement capacity that you didn’t recognize was lost. This is because the brain naturally creates a blind spot to the areas of our body we do not have access to.
Like all worthwhile endeavors, we must invest time and energy, and movement is no different. What you’ll find in joint flossing is that on the front end you must invest more time in skill development, however, the payoff is a greater expression of those skills on the backend. Your health and vitality will become more sustainable with this attention to the minimum daily requirement of quality movement.
Join Joseph on Friday, April 17 at 10:00 am MDT for a 2-hour Manual Muscle Testing Redefined mini seminar on nervous system response. In this seminar you will learn how to vet the two false positives and negatives that are influencing binary MMT.
In February I had the honor of sharing my craft with a great group of practitioners. We had an international crowd. Physical Therapists, Chiropractors, movement therapists, and massage therapists all came together to learn how to appropriately assess and interact with the breathing apparatus.
Our host John Goldthorp works with accomplished athletes at Fix Your Run in Philadelphia. I met John 7 years ago at an Anatomy in Motion seminar in NYC. John and I have stayed in touch over the years, and when the opportunity to share Dynamic Neuromuscular Assessment, I was happy to come out and share my craft.
John and I share many of the same philosophies of movement and training. One aspect of this is how we interact with our clients to co-create an experience.
Here’s what John has to say about his experience:
“Recently, I had the pleasure of taking Joseph Schwartz’s excellent Dynamic Neuromuscular Assessment™ Module 1 seminar. To say there were a few a-ha moments would be a massive understatement; they kept coming, seemingly a few every hour. While that may sound overwhelming, the way the course was structured allowed for plenty of hands on time to synthesize the new information.
I personally experienced the power of this work during the course, having observed my body measurably change in the roughly 5 weeks since I attended, and would love to share with you my experience.
Two years ago, I experienced a ruptured appendix which required an extensive surgery and recovery period. This was certainly a major trauma to my body, but I have been able to recover and get back to – and even exceed – previous levels of performance thanks to the help of many of my movement assessment colleagues.
However, despite making quite a bit of progress in the first year post-surgery, I seemed to have plateaued in terms of my diastasis recti even though I’d been diligent with breathing and strength work.
As Joseph was teaching, I naturally began to wonder, “Is there a prime driver in my situation? Is there a reason my diastasis, although improved, was resistant to further improvement?”
DNA™ teaches you how to have a conversation with the nervous system so that you can determine the prime driver of a compensation.
Perhaps the biggest takeaway of DNA™ is that in order to assess accurately, one must “keep the container safe.” In other words, as my colleague Shannon Connolly so brilliantly stated, “you have to treat the central nervous system with respect. We have to remember that we all have developed coping strategies in order to protect ourselves. Just forcing a modality like a soft tissue release or specific movement/pattern onto someone just because it is “tight” or “feels good” when their nervous system is not prepared for it or cannot cope with that strategy can actually make things worse or keep driving the coping mechanism.”
A ruptured appendix – was it just a structural trauma? Of course not.
DNA™ enlightens us to become aware that a prime driver of movement compensation can be structural, physiological, or emotional in nature and each will affect the other.
During the course, I was chosen to be a breathing assessment demo for the class. Despite having a wealth of knowledge about breathing – and doing my best to breathe properly – I ‘failed’ a majority of functional manual muscle tests involving the breathing apparatus. Now, this wasn’t a huge surprise as I did still have a noticeable diastasis recti, but I couldn’t wait to find out WHY. What was my prime driver, the parking brake holding me back from making more progress?
During the assessment many tests improved when I touched (therapy localized) the scar, however, not all of them.
Assessment showed the prime driver in my case was a limbic association with the ruptured appendix experience. In fact, it was determined that it was the fear experienced after I learned I would need surgery which was the underlying limbic association. Think your breathing might change in response to fear? You’d better believe it. I was ‘stuck’ there, breathing inefficiently, ever since.
We cleared that association using a tool called ‘self rescue’ (just like releasing tight muscles, there are many tools useful for limbic associations) and retested. ALL breathing apparatus tests were now functional. I took my first truly functional breath in two years.
I’m excited and pleased to report it has been roughly 5 weeks since the course and I’ve seen the size of the diastasis recti decrease noticeably for the first time in about a year!“ — John Goldthorp
Thank you John for sharing your experience! I’d like to take a moment and share how The FiveTenets of DNA™ are so potent in providing the nervous system with the optimal environment for beneficial learning.
The Five Tenets of Dynamic Neuromuscular Assessment™
Keeping the container safe is perhaps the most important aspect of the practitioner-client interaction. How we stimulate and tone down the nervous system of our client has a profound effect on the outcome of our interaction.
We utilize the premise that the nervous system learns coping strategies as a means for safety and survival. Those coping strategies have a purpose. How we determine if it is safe to displace a coping strategy with a more beneficial or optimal option is an important aspect of our interaction with the nervous system.
Technique-based therapeutic interventions do not consider whether it is safe to remove a coping strategy. Instead, the application of technique-based interventions is based on whether symptoms change or not. Without considering why the nervous system has utilized a set of coping strategies, can produce undesirable effects by trying to change them. For example, when our client’s return over and over with the same symptoms, or their symptoms worsen, this illustrates that the coping strategy has not been appropriately addressed.
There is an alternative to a technique-based intervention. This requires a specific process to identify the Prime Driver of the coping strategy so that the driver can be appropriately addressed.
~ Manual muscle testing can and will produce skewed results
This is the elephant in the room. Traditional manual muscle testing has some inherent problems. I’ve identified two false negatives and two false positives within the binary context of MMT.
However, there’s no need to throw the baby out with the bathwater. Instead we can employ a specific process to have non-binary conversations with the nervous system. This starts with autonomic nervous system response. We know that the receptor’s response changes when the parasympathetic up-regulates to the sympathetic nervous system. This becomes the first step in creating a tangible benchmark in movement assessment.
The ANS response is an indirect movement assessment. This is then combined with a direct movement assessment. These two aspects of the assessment process sophisticates the faulty binary approach to a more accurate non-binary conversation with the nervous system.
~ Global / Local / Global
Global movement engages feed-forward motor planning. This gives the nervous system the opportunity to utilize its preferred coping strategy. Once that coping strategy is stimulated by movement, we can dissect the individual building blocks of that movement. This allows us to go deeper and more effectively in the assessment process.
~ Secondary Compensation distracts us from the Prime Driver
Secondary compensation is the low hanging fruit we see in our clients symptoms. Our primary coping strategies require resources. The symptoms clients are experiencing have a correlation to giving up the resources needed by the prime driver. If we remove the option for those resources, we are creating a safety issue for the nervous system. This is counter to keeping the container safe.
~ Specific Adaptation to Imposed Demand, the SAID principle is our ally in efficiency
The SAID principle affects the outcome of corrective strategies. How the nervous system is cued with the symptom causation relationships, builds the internal kinesthetic picture of the nervous system’s coping strategies. When the dots aren’t connected for the nervous system, it may or may not be to make the connection between correlations and symptoms.
This is why the mapping process I teach in DNA™ is essential to honor these five tenets. In DNA™ Mapping, we derive the common denominator, the prime driver. We then evaluate the prime driver. We then can simply do one intervention that resets the whole paradigm of prime driver, main pair, and secondary compensations. In John’s experience, the combination of the limbic association and the structural adaptation from surgery had to be appropriately interacted with so that the nervous system had the opportunity to reset all the players in respiration. When the nervous system can respond appropriately, the structure can follow. The result is his diastasis recti can now mend more fully.
For every symptom you’re seeing come into your office, there is something driving that symptom. It may or may not be obvious. These symptoms are a coping strategy that the nervous system perceives as necessary for safety. In addition, coping strategies require resources to sustain. An often overlooked and underappreciated element of assessment is asking yourself two questions: 1) Where do those resources come from? 2) Are those resources in sustainable supply?
By the end of this article, you’ll have a fresh lens that frames adaptation and coping strategies. This reference will help you better evaluate, assess and treat your clients so that their nervous system has the optimal opportunity to make lasting change.
Let’s look at the universal principle of homeostasis to further gain understanding how the nervous system is allocating and engaging resources.
The universe is made up of atoms. Atoms can have many configurations and combine in multiple ways. The periodic table of elements gives us insight into the many ways atoms are expressed. The construct of the atom is the building block of matter. Atoms have a balanced charge of positively charged neutrons and negatively charged electrons — homeostasis! The balance of these charged particles are the blueprint for how atoms assemble into larger structures. Atoms have the same number of protons as electrons. When an atom is missing an electron, it is called a free radical. “The unpaired electron makes them unstable and highly reactive. In a process called oxidation, free radicals steal electrons from other molecules.”
Our neurology follows a similar pattern of homeostasis. When one of our systems has a need, that need requires resources. The nervous system acquires these resources from an available donor – it is a reciprocal partnership.
Reciprocal Partnership
Our neurology is affecting our breath, movement, and structure. These are the more tangible elements of the interdependent body systems. Reciprocal partnership — homeostasis — is affecting each and everyone of these systems as well. Let’s first look at how this is reflected in the musculoskeletal system, and then we can open up the lens.
One commonly known example of reciprocal partnership is the reciprocal inhibition. Reciprocal inhibition is a function of how muscles behave in the musculoskeletal system. Reciprocal inhibition can be defined as when muscle response increases, the functional opposite muscle response will decrease. For example, when we do a bicep curl, our tricep must relax so that the bicep is not competing with the tricep when moving the weight.
If we didn’t have this fundamental principle in movement, the muscular system would be constantly competing for energy.
This same principle applies to the parasympathetic and sympathetic nervous system. When the sympathetic nervous system becomes stimulated, or up-regulated, the counterpart, the parasympathetic down-regulates. Homeostasis happens in every system of the human organism.
Let’s apply this template to a therapeutic setting using events, adaptation, and prime drivers.
Events
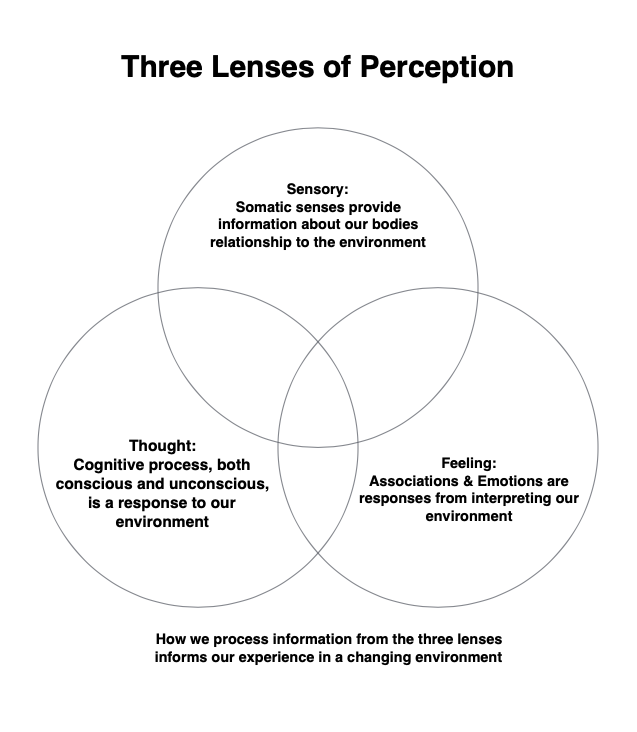
An event is an experience someone has involving multiple elements including perception, sensory, feelings, and thoughts. Each of these lenses contribute to how an event is then interpreted and registered by the person’s nervous system.
Adaptation
An event and adaptation are intrinsically linked. Adaptation is a learning process of the nervous system to cope with and respond to the changing environment. Adaptation has three characteristics: beneficial, neutral, and maladaptive. The adaptation that occurs during an event is perceived by our nervous system as necessary, as its job is to keep us safe.
Prime Driver
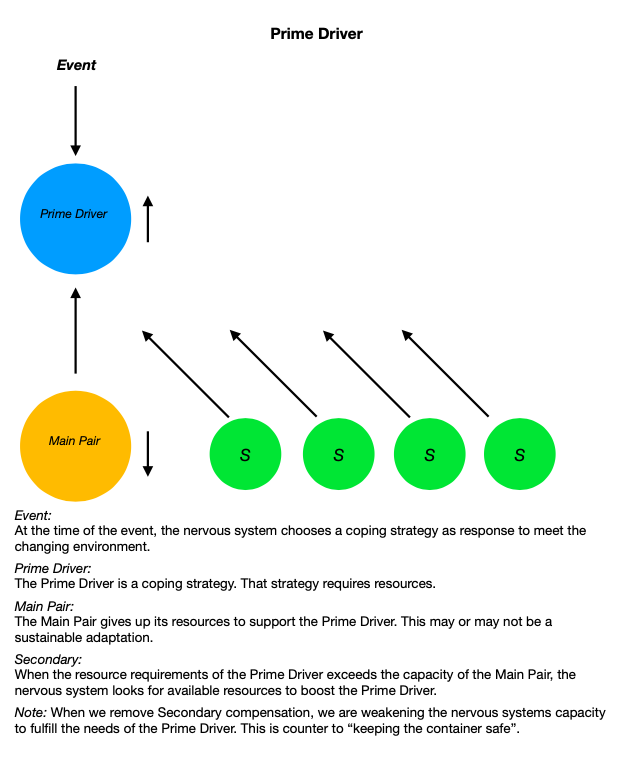
The prime driver is the first element the nervous system utilizes during an event. The prime driver requires resources to function. As the prime driver’s needs increase, the resources of its reciprocal partner are decreasing. The reciprocal partner is giving up its resources in order to boost the resources available to the prime driver. This is mirrored by the example of reciprocal inhibition.
The prime driver is in a reciprocal partnership with another element. This element is giving up its resources to boost the prime driver. We will call this second element the prime driver’s main pair. Now, what do you suppose happens when the prime driver’s main pair no longer has sufficient resources to maintain the relationship? The prime driver looks for another element that can give up its resources. We will call this a secondary. There is the potential that there are many secondaries that are supporting the prime driver. As the needs of the environment increase, the needs of the primary driver to maintain sufficient response increases as well. Environmental load, and the coping strategies to meet that load, are affecting how our nervous system is responding.
Nervous System Response
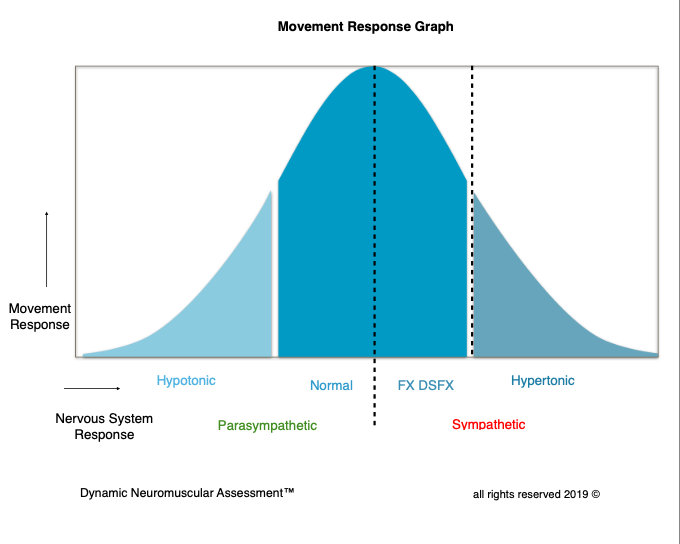
Under a low load context, our nervous system should have capacity to remain normally responsive. As our environmental load increases, we should have capacity to appropriately respond to those needs when required. Sometimes this includes the need to up-regulate. Then as the stimulus of the environment ceases to require that up-regulated response, the resources requirement then down-regulates or returns to a normal response. When it does not, this is referred to as a hypertonic response. A hypertonic response is a coping strategy.
Muscle response gives us a tangible benchmark for how our nervous system is responding to a changing environment. This can be qualified by the conversation received by the afferent signals from peripheral receptors. Our receptor response changes when the nervous system upregulates from the parasympathetic to the arming of the sympathetic nervous system. The muscle response graph gives us insight how the nervous system is responding to environmental load. This is a key element in the assessment process. Rather than treating a symptom or toning down the symptom, in order to really help our clients, we must identify the specific stress that is creating inappropriate movement response and specifically what the nervous system needs to restore parasympathetic homeostasis.
Limbic System
The limbic system is the primary information gathering and response center in the brain. It receives a portion of neurological inputs from our environment that are the perceived experiences that are then processed and collated. This is so we can respond to these inputs in real time. The limbic system is commonly known as the emotional center, in addition to the function of memory, autonomic regulation, and motor control. Associations and the correlating emotions to those associations have an effect on both autonomic regulation and motor control.
The Limbic Associative Feedback Loop (LAFL) demonstrates how coping strategies work.
Event:
We live in a changing environment and our somatic sensory pathways are constantly monitoring and taking in information. Each instance potentially becomes an event.
Neurological Inputs:
Events are registered through somatic sensory pathways. This information is both conscious felt sense and our unconscious unfelt sense.
Association:
When we receive new somatic sensory information, the limbic center looks for something similar that it can attach to the new information — past events inform the present moment.
Processing:
At this juncture, the limbic center processes both the somatic sensory information and the association. That information is then directed to different parts of the brain depending on where that information falls in the spectrum of “need to respond” in a survival based hierarchy.
Neurological Output:
A person’s response to an event is based on multiple factors. Their ability to appropriately respond to the stimulus of an event is based on conditioning and the relationship to adaptation. Additionally, depending on the perceived survival need, the spectrum of the response will come from the amygdala, prefrontal cortex, cerebellum, or brain stem. This output becomes the next potential event. Receiving information from our environment and responding to that information becomes a perpetual loop.
What LAFL Looks Like:
A person experiences an event by receiving neurological inputs into the limbic system. There is now a need to respond. The limbic system begins looking for similar neurological inputs to this event and how it has previously responded to those inputs. That coping strategy has a prime driver. In order to create homeostasis, there will be a main reciprocal partner as well as the potential for multiple secondaries. As the need for the prime driver increases, multiple secondaries can create a multi-symptom presentation.
What if the event is a novel experience? In the future, that novel experience will become a new association along with new coping strategies utilized to respond to a similar set of circumstances.
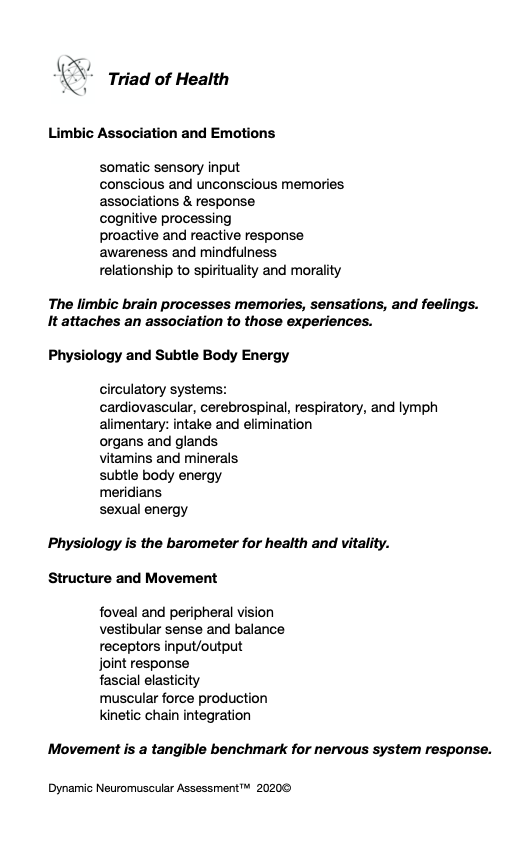
The nervous system has a full palette of options it can utilize as a prime driver at the time of the event. It can be structural, physiological, or limbic . Likewise, the nervous system can choose a main pair and subsequent secondaries from the same palette. This pallet is generalized in the Triad of Health chart.
Good Intentions – Wrong Approach
One of the common problems to recognize in the assessment and treatment of the musculoskeletal and its corresponding motor control systems is that therapists are frequently treating the symptoms. This is problematic because often those symptoms are being recruited by the nervous system for a reason. Without adequately vetting why those symptoms are present, we can inadvertently remove a necessary coping strategy. This can create vulnerability in our client’s nervous system. When we apply the universal principle of reciprocal partnership, we can be more efficient therapists. Instead of treating the low hanging fruit of the symptom, we can follow the symptom-causation relationship to derive the prime driver. When we appropriately address the prime driver, not only do we accomplish more in helping our client’s presentation, we are also honoring the primary coping strategy of their nervous system, keeping the container safe.
Let’s take a look at some examples of how the nervous system may choose to support a reciprocal relationship. As manual therapists we may be familiar with how joints and ligaments affect muscle response. Ligaments will act as neuromuscular switches for the muscles that would act on that ligament. When joint position is compromised by load, speed or vector, the ligaments role is to protect that joint. When a ligament becomes strained, it sends input signals to the cerebellum to inhibit the muscles that would act upon that joint/ligament. This is a non felt sense protection mechanism. The strained ligament will look for a reciprocal partnership to sustain this protective adaptation strategy.
An example can be applied to the knee. If during movement, the ACL gets stressed and the stress load is sufficient enough that the receptors are unable to return to a normal resting response, the movement that caused the knee to deviate into a position that stressed the ACL would be the event. The response to this event is the up-regulated receptor response to the cerebellum. The cerebellum then instructs the assisted muscle to inhibit as a protective strategy. Next, the nervous system looks for a reciprocal pair for the main driver, the strained ACL. Often in structure, the nervous system picks functional opposites. For example, the oblique popliteal ligament has an opposite function in the rotary capacity of the knee.
The low hanging fruit are the muscles that are inhibited. But there is a big problem if we then strengthen those muscles, as the action on the knee is going to increase the already hypertonic response of the ACL. This is treating the symptom! Instead, we need to derive the prime driver and cue that driver to its main pair. When the nervous system receives that information, the cerebellar response is normalized and the associated muscles return to normally responsive.
Prime drivers that are of the emotional association nature will often pair with an organ. The resources needed by the emotion is given up by the organ. A few classic examples are anger/liver and worry/stomach. The rub is if we remove the secondary compensations without addressing the prime driver, we are potentially weakening the ability of the prime driver to maintain its resource needs.
When we remove a coping strategy of the limbic system, the nervous system goes on alert with a sympathetic response. Further, depending on the spectrum of the association, mild to severe, this can be destabilizing and highly counter productive. In the severe spectrum, this can cause a PTSD episode. This is why we must evaluate the source and causation of the imbalance we are seeking to treat, before treating symptoms in the musculoskeletal system. This is how we move into being a master in our craft regardless of the corrective tools we deploy.
Let’s look at a Dynamic Neuromuscular Assessment™ Module One case study to further illustrate the concept of the prime driver.
Case Study: Assessment of the Breathing Apparatus
Global Skill: QiGong Posture
Visual: appears that the diaphragms move out of alignment creating a lack of integrity in the core cylinder
MMT: Functional Dysfunctional Response: Correlation to Limbic Association
Limbic Association TL- same association as the global movement association
Double Check Work:
Client TL’s the R Jaw
Retest PF and L sub-occipitals
Normal Response
Corrective:
Cue the associated movements into the nervous system (order matters)
Limbic hold on the Bennett points (cranial hold, observe the breath)
Retest: (in the same order)
PF normal response
Sub-occipitals normal response
Jaw normal response
Re-insert local components back into the Global Movement
Normally Responsive
Summary:
As body helpers, our first consideration is client’s safety — what I like to call keeping the container safe. We did this by adding stability into the system. We did not remove coping strategies which would result in creating vulnerability to the system. The old MMT paradigm would indicate that we should have released the sub-occipitals. If we would have tried to correct a dysfunctional component correlated to a limbic association, potentially the response of that limbic association would have increased. That would have resulted in harming the client!
Limbic associations can have multiple layers mirroring the template of compensations with primary and secondary/s, so we had to tone down the association so that the nervous system could appropriately respond to the environment. There may be more work needed to effect sustainable change over time. However, with one corrective, we restored movement function to all the local components and the initial global assessment. That could not have happened if we did not utilize the SAID principle, specific adaptation to imposed demand, in our assessment and correction strategy.
If you’re not fully vetting your client’s presentation, you may be taking them down a path you don’t need to travel. Mapping is an essential tool in your toolbox to avoid wasting valuable resources and time for both you and your client.
Often times, practitioners are treating their clients before they know the root source of their client’s presentation. Not only is this a waste of time for both the client and the practitioner, it may also mean they end up treating the symptoms of secondary compensation. This can be a perceived threat to the nervous system and lead to further layers of compensatory adaptation down the road.
When I started implementing mapping into my own assessment, here’s what happened.
In the past I would evaluate movement response and look toward what was needed to restore that response. This was a method of looking for the low hanging fruit with the hope that it would make a tangible difference. The process was hit or miss at best. As I became a more adept practitioner, I wanted to understand why I had the misses. I started taking more time in the assessment process. I also started to look for the common denominator that was correlating to the inappropriate movement response in my clients. Then I would assess that correlation. It took longer to assess, but that investment in time was more than made up for in the optimization of the corrective strategies that were utilized. Instead of multiple correctives to the nervous system, I was only using one or two laser focused interventions. I found people were getting faster results with minimal stimulus to the nervous system, because it was the right stimulus.
When you implement an assessment process that honors the nervous system’s need for safety, you will begin to see an optimization in your assessment — a leveling up so to speak. This starts with building safety into the nervous system by not removing coping strategies that have been put in place for a reason.
In order to do so effectively, we need to understand why the nervous system has organized the coping strategy that is being presented. I call this mapping. In mapping, particularly through the lense of Dynamic Neuromuscular Assessment™, we are evaluating the symptom-causation relationship. When evaluating the symptom-causation relationship, we have to keep in mind that the causation of one set of symptoms may be a symptom of another causation.
Let’s use a recent pelvic floor client assessment to illustrate the symptom-causation relationship. After doing a thorough movement assessment process, I found the movement functions that did not respond appropriately correlated to a ligament in the coccyx. I then evaluated the ligament in the coccyx. This assessment correlated to a limbic association.
If I would have spent valuable time working directly with the ligament, it could have been problematic for a number of reasons. One problem could have been that the limbic association would have trumped any structural change that might have happened temporarily. Another problem, and more potentially detrimental, is a safety issue for the coping strategy that the nervous system put in place to support the limbic association. When we remove that coping strategy as an option for the nervous system, that potentially can create instability in the limbic center’s ability to cope with the association. This can derail a person’s capacity to appropriately respond to their environment.
In this example, the limbic association required support from the structure. That support is a resource. If we remove that resource, the nervous system will come up with a strategy to replace that resource. The best case scenario is that the nervous system recruits a similar or familiar coping strategy. The worst case scenario is that things could take a turn for the worse with the nervous system replacing that resource with a less desirable coping strategy than its original choice. This could be a structural, physiological or even a limbic maladaptive strategy.
If you’ve ever had clients that either did not respond to treatment or had their symptoms return, this is the reason why: The root source of their presentation was not addressed appropriately, so when day to day activities loaded their nervous system, their symptoms got worse and/or were compounded by a new coping strategy. This is when utilizing mapping in our assessment is critical to derive appropriate intervention with the nervous system of our clients.
Would you like to learn how to optimize your assessment and utilize the process of Mapping to help your clients in a profound and efficient way? Dynamic Neuromuscular Assessment™ is a method by which to have a conversation with the nervous system through movement. Our next DNA™ Seminar is February 22-23rd in Philadelphia. Hosted by John Goldthorp of Fix Your Run.
The pelvic floor is often overlooked and misunderstood during movement assessment. The pelvic floor is integral to both breath and movement. This is good news, as it allows us to use movement to assess the pelvic floor. This is important because of the sensitivity of the pelvic structure. More invasive approaches like direct palpation of the pelvic floor compromises safety of both practitioner and client. Starting with movement assessment builds safety in the nervous system. In addition, movement assessment also allows pelvic floor assessment to be accessible to practitioners where direct contact with the pelvic floor is out of their scope of practice.
There are a few principles of movement assessment to consider with pelvic floor assessment. These include functional assessment, the biomechanics involved, and how to keep the container safe. Differentiating how the nervous system is responding from structural response becomes the foundation of functional assessment. Next, we need a clear understanding of the biomechanics involved. Because the pelvic floor is fundamental to the breathing apparatus, the pelvic floor is virtually participating in every possible movement. And perhaps most important, how we keep the container safe. The pelvic floor is a sensitive, limbically driven, aspect of our structure, and we must use caution so that we do not overstimulate the nervous system.
From my perspective, there is currently a fundamental problem in the manual therapy community. Manual therapy is predominantly a tool-based intervention strategy; consisting of many variations of tools and techniques. As a result, practitioners take the particular tool they’ve been educated in and apply it to the presentation of the client.
Being a former race car mechanic, I liken this analogy: If I purchase a brand new shiny 10mm wrench, am I going to go around the car and look for fasteners it might fit? That doesn’t make a lot of sense, does it? Let’s dive a bit deeper.
We see a plethora of technique-based courses being offered in our profession. There are many reasons why we need to have an array of tools available to us. However, the tools themselves often distract us from finding the causation of each unique presentation. When we are simply applying a tool to a problem to see if the problem changes, we are guessing. This has the potential to be negligent.
I recognize that the statement that a tool-based intervention is potentially negligent is a bold statement. Let’s build some context that supports the statement. We need to consider two specific variables in an individual’s presentation.
Adaptation
Adaptation is a learned coping strategy. Understanding why that coping strategy was implemented by your client’s nervous system is the primary consideration. That person’s experience has biopsychosocial factors that influence how their nervous system chose to cope with and adapt to the changing environment around them.
Compensation
The combination of symptoms based on a nervous system’s chosen adaptive strategy, is not consciously chosen. It is instead a function of the survival-based nervous system. Adaptation is mostly unconsciousness behavior. However, there are exceptions when we consciously add elements to our environment for beneficial change — like changing one’s diet or engaging in a fitness plan. Maladaptive compensations are often driven by our unconscious, even if it seems like we are making conscious choices.
Here’s a hypothetical presentation that illustrates how a tool-based intervention can be negligent. Let’s use an example of regional interdependence, where one region of the body compensates for another region of the body not participating. For example, a client comes in with sacroiliac pain. The function of pelvic sacral stability is diminished in some way. Using the model from Lovett Reactors, the therapist traces the instability to the jaw. The therapist then treats the jaw.
There is a fundamental problem with this. While the pelvic sacral stability issue is a symptom of the jaw, more times than not, the jaw is a symptom of something else. That something else is related to an experience, which became an association that has an array of emotional responses. The symptoms we are seeing in the jaw is related to a past experience and a limbic association. Effectively, what the therapist has inadvertently done is remove the coping strategy of the limbic system. The potential for this to blow up is pretty high.
Now let’s look at a real life example. This occurred in a seminar that I attended several years ago. A combat veteran was getting a neurological treatment from a colleague to correct a movement dysfunction. Unbeknown to the therapist, that movement dysfunction was related to a combat experience. The person on the table had a full blown PTSD incident while being treated. Afterward, he became suicidal and had to be on suicide watch while his limbic system reorganized to find a new coping strategy to compartmentalize the traumatic event.. This kind of response can happen on a spectrum from mild to full blown PTSD flashback like this example. When we are treating symptoms, we are potentially creating a vulnerability in the coping strategy of the nervous system.
There is a solution to this problem of tool-based therapeutic intervention. The solution is an assessment-based process that determines the root cause of the individual’s presentation. That assessment process must consider each aspect of the presentation as a potential symptom. The symptom-causation relationship must be traced to the driver of those symptoms. That driver is the root causation. That assessment process must take into consideration the entirety of the biopsychosocial model. The down side of this is when the causation of the individuals presentation gets out of our scope of practice. This is when our referral network becomes very important.
As therapists, we can do better. We can advance from being the hammer and seeing every problem as a nail. Instead, we can hone our assessment strategies to derive the appropriate tool that is needed — see The Five Tenets of DNA™ to learn more. We can determine if it is safe to use that tool. We can live up to the first rule of the Hippocratic oath: Do No Harm.
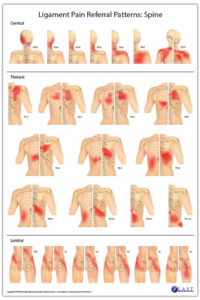
I was recently asked to review Robert Libbey’s new ligament referral charts. This is an important contribution to the therapeutic community. I’d like to detail a few reasons why understanding ligament function and pain referral is important in consideration for structural-based pain and maladaptive movement strategies.
Robert Libbey’s Ligament Pain Referral Pattern Posters
The area in which we sense pain is often not the source of that pain. More often than not, therapists are trying to treat the muscles around the symptom of pain. This yields inconsistent results. Muscles aren’t always the source of the pain. Muscular behavior, tonicity, and recruitment patterns are based on the response from the brain’s motor control systems.
Ligaments trump muscles in the survival-based nervous system. Ligaments act as neuromuscular switches to increase muscle tone or decrease muscle tone. This reflects the neuromuscular relationship in movement called reciprocal inhibition. Reciprocal inhibition allows for muscles to act as a team. As one muscle activates or increases its energy output, its reciprocal partners deactivate or decreases their energy output. This fundamental principle is a primary function of ligaments providing somatosensory input for the nervous system to process and respond to.
Ligaments act as a safety valve in joint response. Ligaments also inform neuromuscular sequencing. When a ligament is stressed, strained or otherwise impaired, the afferent input signals that ligament sends to the cerebellum, switches off, or inhibits the muscles that would act on that ligament. This is a protection strategy so that joint movement does not further stress the impaired ligament. The impaired ligament does not need to be injured to send signals that would result in an inhibitory response. The result however, would mimic an injury. These errant neurological input signals can be reset with appropriate manual therapy intervention.
Ligaments have two primary roles:
Ligaments hold joints together in their optimal position. As joints move, muscles respond to that movement. When joints lose their optimal alignment, the muscles function that would act on those joints becomes impaired. The musculoskeletal system needs appropriately responding muscle function to control movement, to keep the structure safe.
Ligaments provide somatosensory input to the brain’s motor control systems. This sensory input allows for non-thinking movement. We do not have to think about which muscles to activate when we move. The afferent information from ligaments, and other receptors, provide the field of awareness for the brain to respond. We would not be able to manage the complexity of walking and running if not for the information that the ligaments provide.
Here is an interesting fun fact about the somatosensory aspects of ligaments. There are two tracts of afferent information that goes from the peripheral to the central nervous system. The first tract, the spinothalamic tract is received in the limbic center’s thalamus. This information is processed and informs our kinesthetic awareness. This is the conscious field that is often referred to as proprioception. The second tract, the spinocerebellar tract, particularly has my interest. The majority of information that is received from the periphery directly to the cerebellum does not inform our conscious kinesthetic awareness. This is how movement occurs in the non-thinking place. The nervous system is responding to the changing environment without that person’s conscious volition .
Ligaments, both their assessment and treatment, have an essential role in the structural therapist’s approach when working with clients. These important charts published by Robert Libbey, RMT, provide a visual reference to look deeper than the symptoms of pain. These are another set of complementary charts to add to your collection – Complementary Reference Tools.
The concept of using movement to floss the connective tissue that surrounds nerves is not new.
Let’s open the lens beyond nerve flossing and look at how other aspects of our structure benefits from flossing as well.
Tissue Flossing/Pulping:
This is movement that specifically targets fascial compartments. Co-activation of functional opposites creates spirals in the fascial compartments. This effectively wrings out the tissues like wringing a wash cloth. The benefits of pulping the structure are many. Releasing residual muscle tension, squeezing and soaking the tissues in fluid exchange, restoring elasticity in the tissues, and muscular integration are important aspects of pulping.
Joint Flossing:
Joint articulation or joint mobility also has many benefits. Joint mobility is not passive. There is the co-activation present though not as intense as in pulping. The intention is to move the structure through its complete range of motion in a smooth, controlled, pain-free manner. Each joint has its unique attributes in movement. The Functional Compass™ – as outlined in Applied Anatomy for Yoga Therapeutics – provides a map for movement potential.
One distinct quality of joint flossing is working on the capacity to isolate movement to a targeted joint. This develops the individual building blocks of movement. When we have motor control of the individual building blocks of movement, these building blocks can then be assembled into larger integrated movements.
The nervous system will always look for the most efficient way to accomplish movement. The more choices that are available, translates into more options for efficiency. Also, when movement deviates in a changing environment, the nervous system can then maintain a safety valve with all the options available. The nervous system knows which movement options are available and which ones are not. The nervous system will always devise a way to work around movement options that are not available. This is a fundamental of maladaptive compensation.
Benefits of joint flossing; Joint articulations:
– renew synovial fluid in the joint capsule.
– disperse joint salts and metabolic by products.
– are a beneficial stimulation for the nervous system.
– develop the building blocks of movement.
– stimulate mechanoreceptors.
– cue the nervous system for the available building blocks of movement.
– are a form of active recovery.
– prime the nervous system for work load.
Something to consider:
In real life, there are no warm-ups. When the demands of a changing environment requires response, either the capacity to respond appropriately is available or not. Only during our training time do we have the luxury of warming-up and skill development. While it may seem pedestrian to practice joint mobility as a regular aspect of your training program, I can say as an aging athlete, it is fundamental to maintaining healthy structure and movement.
By streamlining assessment via the considerations outlined in Dynamic Neuromuscular Assessment™ Seminars, you can save yourself and your client a lot of time and energy. Let’s illustrate this with several of the considerations that make DNA™ unique.
First Consideration: Keeping the container safe
DNA™ teaches us effective ways to monitor the response of our client’s nervous system in order to keep the container safe. Our nervous system chooses adaptation strategies as a protection mechanism. These strategies have a priority. There is the primary compensation and the potential for multiple secondary compensations. These secondary compensations boost the primary compensation. If we indiscriminately remove a secondary compensation, we are inadvertently creating a void in the container of our client’s coping strategies. The nervous system then must adapt to not having that available element. What the nervous system chooses to fill that void with may potentially be more maladaptive than the original coping strategy. This can happen in all three categories of the trine in Applied Kinesiology: movement and structure, physiology and subtle body energy, and limbic associations and emotions. The danger here is that if we kick out the leg in a three-legged stool…something is going to crash. This can become a big problem if the nervous system chooses to utilize the energy system from our physiology or limbic associations to bolster dysfunctional movement.
Second Consideration: Manual Muscle Testing can and will produced skewed results
Protocols we utilize in Dynamic Neuromuscular Assessment™ allow us to recognize when the false negative and the two false positives show up in MMT. There are two causes for this. First, the practitioner may have unresolved issues in their mind/body. As practitioners, we affect the outcome. Our expectations and projections, conscious and unconscious, have an impact on the testing results. The second cause is the response we are getting from the client. There are two false positives and one false negative that are constantly showing up in our MMT. If these are not vetted, our correlation of relationship and causation will be skewed. We need a specific process, or protocol like what is shared in DNA™, to double check when the movement response gives us faulty data.
Third Consideration: Global / Local / Global
Global assessment in DNA™ evaluates the ability of the nervous system to respond using feed-forward assessment. This allows the nervous system the opportunity to utilize the primary compensation. Then we can further vet the dysfunction by looking at the local components. The first global assessment gets us in the right neighborhood, the local components, or building blocks of movement, gets us to the right house. As we continue with the process we end up in the right room, in the right house in the right neighborhood. After we have vetted the primary driver, restored normal response, we can insert that back into the global movement for re-evaluation. The global local global approach is much faster at vetting the primary compensation. This is the opposite of the hit or miss strategy of relying on local assessment to resolve a presentation.
Fourth Consideration: Secondary compensation leads us astray from the primary driver
When we are evaluating movement, every dysfunction has the potential of multiple pieces. How we trace, or map, the dysfunctional components in DNA™ makes a difference in the outcome for your client. We must treat each piece as a potential symptom and completely vet the presentation before we employ a corrective strategy. This relates back to the first consideration and is a major tenet of DNA™, we do not want to remove a secondary coping strategy as that creates vulnerability. The mapping process specifically vets the dysfunctions to arrive at the primary dysfunction. Initially this may seem like the tortoise and the hare approach. The hare would be treating what they find as it presents itself. The tortoise looks at the complete presentation before using laser focused corrective strategies that have the most impact with the least amount of intervention.
Fifth Consideration: Specific Adaptation to Imposed Demand, the SAID principle is our ally in efficiency
DNA™ radically optimizes your assessment by implementing the SAID principle. The SAID principle has two primary ways it affects the outcome of our work. The first is the preliminary steps we take during the evaluation process. Does the process complete the map of the presentation? When it does, we can then cue the nervous system to all the elements that correlate to the primary dysfunction. When we employ a corrective, then the nervous system has an understanding of how these pieces interrelate. We then get the most value from the least amount of work. The second way the SAID principle affects the outcome is related to the corrective strategy itself. If we have not cued the nervous system appropriately, then the nervous system must interpret what, how and why the pieces fit together. Often, the nervous system is unable to fill in the missing pieces. When this happens, our corrective strategy will be temporary at best. This is why clients will return with the same presentation over and over. The nervous system is not getting enough information to make a sustainable change. Instead, when the environment load increases beyond capacity, the nervous system returns to a familiar coping strategy.
Let’s look at how these five considerations weave together in an evaluation process. This is an excerpt from a recent DNA™ Module One practicum.
Intention: Assessment of the breathing apparatus
Global Skill: QiGong Posture
Visual: appears that the diaphragms move out of alignment creating a lack of integrity in the core cylinder
MMT: Functional Dysfunctional Response: Correlation to Limbic Association
Local Components:
Sacrospinalis / multifidus – normally responsive
TVA – normally responsive
Pelvic Floor – functional dysfunctional
Vet Pelvic Floor:
Structural – L sub-occipitals TL
Vet L sub-occipitals – functional dysfunctional
Structural – R jaw TL
Vet R Jaw – functional dysfunctional
Limbic Association TL- same association as the global movement association
Double check our work:
Client TL’s the R Jaw
Retest PF and L sub-occipitals
Normal Response
Corrective:
Cue the associated movements into the nervous system (order matters)
Limbic hold on the Bennett points (a generic cranial hold while observing the breath)
Retest: (in the same order)
PF normal response
Sub-occipitals normal response
Jaw normal response
Re-insert local components back into the Global Movement
Normal Response!
Summary:
Using Dynamic Neuromuscular Assessment™ our first consideration is the safety of our client’s nervous system. We then add stability into the system. We did not remove coping strategies creating vulnerability. The old paradigm would indicate that we would have released sub-occipitals. If we would have tried to correct a dysfunctional component that is correlated to a limbic association, potentially the volume of that limbic input would increase. That would have essentially kicked the third leg out of the three-legged stool.
Limbic associations can have multiple layers mirroring the template of compensations with primary and secondary/s. We toned down the association. We did not necessarily remove or clear. We tone it down so that the nervous system can appropriately respond to the environment. There may be more work needed to effect sustainable change.
Using only one corrective – in the DNA™paradigm – we restored movement function to all the local components and the initial global assessment. That could not have happened if we did not utilize the SAID principle in our assessment and correction.
As therapists, our clients come to see us to help them with issues they are experiencing. They often have a clear idea of what they believe is going on. However, we know that the symptoms they are experiencing are often not the root of the issue. Our client’s symptoms do, however, provide us with the necessary clues to arrive at the source of their experience. As therapists, we know maladaptive compensation has a primary causation with secondary supporting players. Often, the symptoms of the secondary compensations lead us astray from addressing the primary causation.
We are familiar with the peeling of the onion analogy. When we are “peeling away the layers” what we are doing is removing secondary compensation from the nervous system’s coping strategy. We are creating a void in the container that could then be filled by unknown element. For example, it is becoming more acknowledged that athletes will perform poorly if their event is after a deep tissue style massage. The reason for this is the global secondary compensations have been removed and as a safety valve, the nervous system puts the brakes on. And if that athlete pushes through that safety valve, strain or injury is the result. Many of us have experienced our clients getting worse after a treatment. The reason why is we removed a secondary compensation without addressing the primary. This left a void in the container and the nervous system filled that void with something, an unknown element.
Let’s unpack this further.
One of our greatest survival attributes is adaptation. Adaptation allows our species to learn from and cope with a changing environment. Without this capacity, human beings would not survive.
There is a universal truth that defines adaptation:
The organism will adapt to its environment regardless of the outcome.
This has far reaching implications on how we adapt to our environment. When we consider short term verses long term adaptation strategy, short-term adaptation may be beneficial. However, as a long-term strategy, the short-term adaptation may not be sustainable and will eventually lead to reduction of optimal function.
The spectrum of adaptation can be further reduced with a second universal truth:
Specific Adaptation to Imposed Demand.
The SAID Principle governs how specifically we adapt to a changing environment. As a survival strategy, it is how we learn to reproduce results with greater efficiency.
When we combine these two universal truths, we can see how our environment, both external and internal, both conscious and unconscious, is influencing our response. We are in a continual process of utilizing coping strategies to respond to our environment. Our coping strategies are learned through the process of adaptation. How we learn from our environment is directly correlated to how we cope with that environment.
When we employ a particular coping strategy, we are reinforcing that strategy. Each time we then use that particular strategy it becomes easier to reproduce. The effect of employing that strategy has three potential outcome categories.
Beneficial:
When an adaptation strategy is beneficial the organism thrives.
Neutral:
When an adaptation strategy is neutral there is no change in the organism.
Maladaptive:
When an adaptation strategy is maladaptive the changes in the organism are unsustainable.
Because these qualities of adaptation are universal, they can be applied to the whole spectrum of our human experience. This includes the triad of Applied Kinesiology; psychology, physiology, and structure.
There is one more universal truth that we need to unpack: keeping the container safe.
The container refers to the collective adaptations and coping strategies that we have utilized in the past. Each one has its own unique signature. Some may be conscious, while others are unconscious.
Keeping the container safe:
Displacing an element with a beneficial strategy keeps the container safe
In the therapeutic process this is of the utmost importance. As a therapist, we cannot simply remove an element from the container, as this leaves a void in the container. That void is then going to be filled with an unknown element. When we are working with a maladaptive strategy, and we remove that maladaptive strategy, what is going to replace that strategy is also going to be maladaptive. To keep the container safe, one must displace a maladaptive strategy with a beneficial strategy. Or at the very least, a strategy that is more beneficial than the maladaptive. This can be applied to our whole spectrum of human experience.
Let’s look at how this would apply to manual therapy. We have heard the analogy of peeling the onion of compensation. This peeling of the onion analogy illustrates that in the adaptation process, there is a root causation with multiple layers on top of or covering up the root causation. Let’s explore this through the lens of adaptation.
When we have learned a maladaptive compensation, the nervous system has a need to make that compensation easier to reproduce. As the needs of the environment increase through frequency, intensity, and/or duration, that learned coping strategy will be challenged. When the nervous system perceives that the present strategy is insufficient to respond to the environment, the nervous system will look for a supporting compensation for the original perceived need. If the environment demands a continual response, another supporting compensation will be added to the equation. As the layers increase, the nervous system does not discern between the need to respond and whether that response is sustainable. This comes back to the first universal truth of adaptation: the organism will adapt to its environment regardless of the outcome.
Said another way, we designate the response to the original causation as the primary compensation. All the other subsequent compensations are secondary. These secondary compensations are put in place by the nervous system to support the primary. As environmental demands increase, so does the need for secondary compensation.
The unknown element that the nervous system chooses to replace a secondary compensation brings up the next concern. The nervous system has a whole palette of systems it can tap into and utilize to support or boost a primary compensation. Compensation is not simply limited to musculoskeletal elements. Compensation occurs in any system within the triad of the emotional, physiological and structural.
When we remove secondary compensation without addressing the primary, we are doing our clients a disservice, as we are not keeping the container safe.
There is a solution for maintaining a safe container. In Dynamic Neuromuscular Assessment™ we share a specific protocol called Mapping. The mapping process identifies and correlates the involved players – primary and secondary – in a compensation.
Only when the global picture of our client’s presentation is understood, can the primary causation be addressed. Don’t simply treat the symptoms, investigate deeper to discern the primary causation.