
Introduction
For every symptom you’re seeing come into your office, there is something driving that symptom. It may or may not be obvious. These symptoms are a coping strategy that the nervous system perceives as necessary for safety. In addition, coping strategies require resources to sustain. An often overlooked and underappreciated element of assessment is asking yourself two questions: 1) Where do those resources come from? 2) Are those resources in sustainable supply?
By the end of this article, you’ll have a fresh lens that frames adaptation and coping strategies. This reference will help you better evaluate, assess and treat your clients so that their nervous system has the optimal opportunity to make lasting change.
Let’s look at the universal principle of homeostasis to further gain understanding how the nervous system is allocating and engaging resources.
The universe is made up of atoms. Atoms can have many configurations and combine in multiple ways. The periodic table of elements gives us insight into the many ways atoms are expressed. The construct of the atom is the building block of matter. Atoms have a balanced charge of positively charged neutrons and negatively charged electrons — homeostasis! The balance of these charged particles are the blueprint for how atoms assemble into larger structures. Atoms have the same number of protons as electrons. When an atom is missing an electron, it is called a free radical. “The unpaired electron makes them unstable and highly reactive. In a process called oxidation, free radicals steal electrons from other molecules.”
Our neurology follows a similar pattern of homeostasis. When one of our systems has a need, that need requires resources. The nervous system acquires these resources from an available donor – it is a reciprocal partnership.
Reciprocal Partnership
Our neurology is affecting our breath, movement, and structure. These are the more tangible elements of the interdependent body systems. Reciprocal partnership — homeostasis — is affecting each and everyone of these systems as well. Let’s first look at how this is reflected in the musculoskeletal system, and then we can open up the lens.
One commonly known example of reciprocal partnership is the reciprocal inhibition. Reciprocal inhibition is a function of how muscles behave in the musculoskeletal system. Reciprocal inhibition can be defined as when muscle response increases, the functional opposite muscle response will decrease. For example, when we do a bicep curl, our tricep must relax so that the bicep is not competing with the tricep when moving the weight.
If we didn’t have this fundamental principle in movement, the muscular system would be constantly competing for energy.
This same principle applies to the parasympathetic and sympathetic nervous system. When the sympathetic nervous system becomes stimulated, or up-regulated, the counterpart, the parasympathetic down-regulates. Homeostasis happens in every system of the human organism.
Let’s apply this template to a therapeutic setting using events, adaptation, and prime drivers.
Events
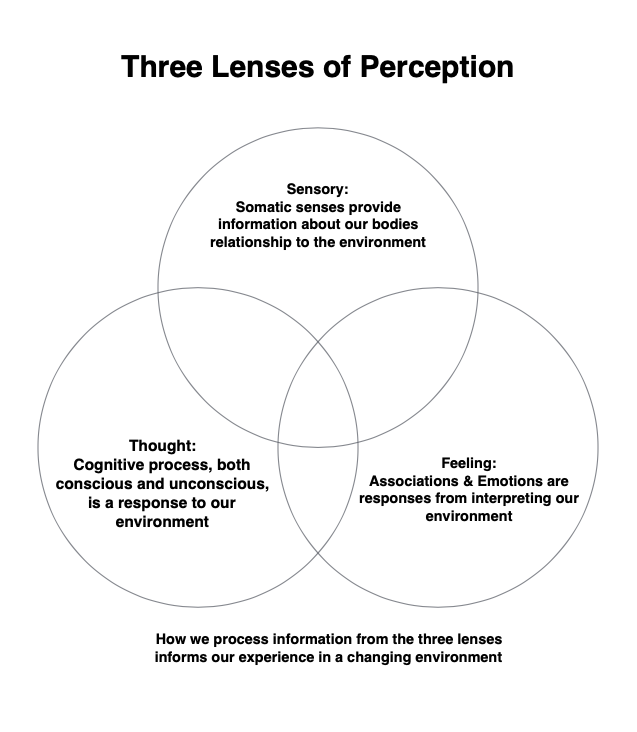
An event is an experience someone has involving multiple elements including perception, sensory, feelings, and thoughts. Each of these lenses contribute to how an event is then interpreted and registered by the person’s nervous system.
Adaptation
An event and adaptation are intrinsically linked. Adaptation is a learning process of the nervous system to cope with and respond to the changing environment. Adaptation has three characteristics: beneficial, neutral, and maladaptive. The adaptation that occurs during an event is perceived by our nervous system as necessary, as its job is to keep us safe.
Prime Driver
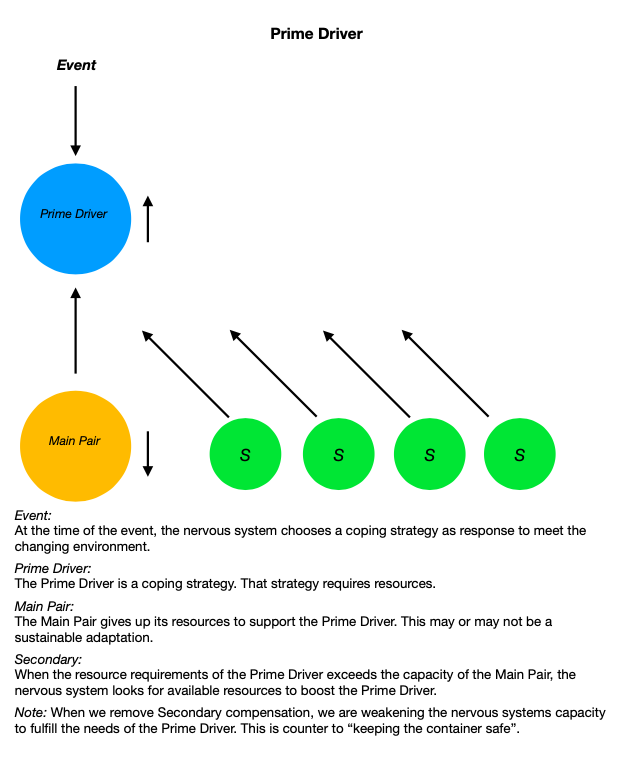
The prime driver is the first element the nervous system utilizes during an event. The prime driver requires resources to function. As the prime driver’s needs increase, the resources of its reciprocal partner are decreasing. The reciprocal partner is giving up its resources in order to boost the resources available to the prime driver. This is mirrored by the example of reciprocal inhibition.
The prime driver is in a reciprocal partnership with another element. This element is giving up its resources to boost the prime driver. We will call this second element the prime driver’s main pair. Now, what do you suppose happens when the prime driver’s main pair no longer has sufficient resources to maintain the relationship? The prime driver looks for another element that can give up its resources. We will call this a secondary. There is the potential that there are many secondaries that are supporting the prime driver. As the needs of the environment increase, the needs of the primary driver to maintain sufficient response increases as well. Environmental load, and the coping strategies to meet that load, are affecting how our nervous system is responding.
Nervous System Response
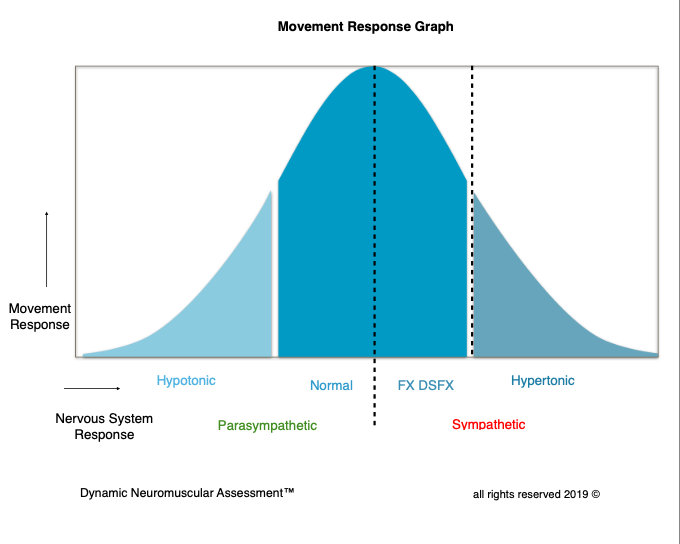
Under a low load context, our nervous system should have capacity to remain normally responsive. As our environmental load increases, we should have capacity to appropriately respond to those needs when required. Sometimes this includes the need to up-regulate. Then as the stimulus of the environment ceases to require that up-regulated response, the resources requirement then down-regulates or returns to a normal response. When it does not, this is referred to as a hypertonic response. A hypertonic response is a coping strategy.
Muscle response gives us a tangible benchmark for how our nervous system is responding to a changing environment. This can be qualified by the conversation received by the afferent signals from peripheral receptors. Our receptor response changes when the nervous system upregulates from the parasympathetic to the arming of the sympathetic nervous system. The muscle response graph gives us insight how the nervous system is responding to environmental load. This is a key element in the assessment process. Rather than treating a symptom or toning down the symptom, in order to really help our clients, we must identify the specific stress that is creating inappropriate movement response and specifically what the nervous system needs to restore parasympathetic homeostasis.
Limbic System
The limbic system is the primary information gathering and response center in the brain. It receives a portion of neurological inputs from our environment that are the perceived experiences that are then processed and collated. This is so we can respond to these inputs in real time. The limbic system is commonly known as the emotional center, in addition to the function of memory, autonomic regulation, and motor control. Associations and the correlating emotions to those associations have an effect on both autonomic regulation and motor control.
The Limbic Associative Feedback Loop (LAFL) demonstrates how coping strategies work.
Event:
We live in a changing environment and our somatic sensory pathways are constantly monitoring and taking in information. Each instance potentially becomes an event.
Neurological Inputs:
Events are registered through somatic sensory pathways. This information is both conscious felt sense and our unconscious unfelt sense.
Association:
When we receive new somatic sensory information, the limbic center looks for something similar that it can attach to the new information — past events inform the present moment.
Processing:
At this juncture, the limbic center processes both the somatic sensory information and the association. That information is then directed to different parts of the brain depending on where that information falls in the spectrum of “need to respond” in a survival based hierarchy.
Neurological Output:
A person’s response to an event is based on multiple factors. Their ability to appropriately respond to the stimulus of an event is based on conditioning and the relationship to adaptation. Additionally, depending on the perceived survival need, the spectrum of the response will come from the amygdala, prefrontal cortex, cerebellum, or brain stem. This output becomes the next potential event. Receiving information from our environment and responding to that information becomes a perpetual loop.
What LAFL Looks Like:
A person experiences an event by receiving neurological inputs into the limbic system. There is now a need to respond. The limbic system begins looking for similar neurological inputs to this event and how it has previously responded to those inputs. That coping strategy has a prime driver. In order to create homeostasis, there will be a main reciprocal partner as well as the potential for multiple secondaries. As the need for the prime driver increases, multiple secondaries can create a multi-symptom presentation.
What if the event is a novel experience? In the future, that novel experience will become a new association along with new coping strategies utilized to respond to a similar set of circumstances.
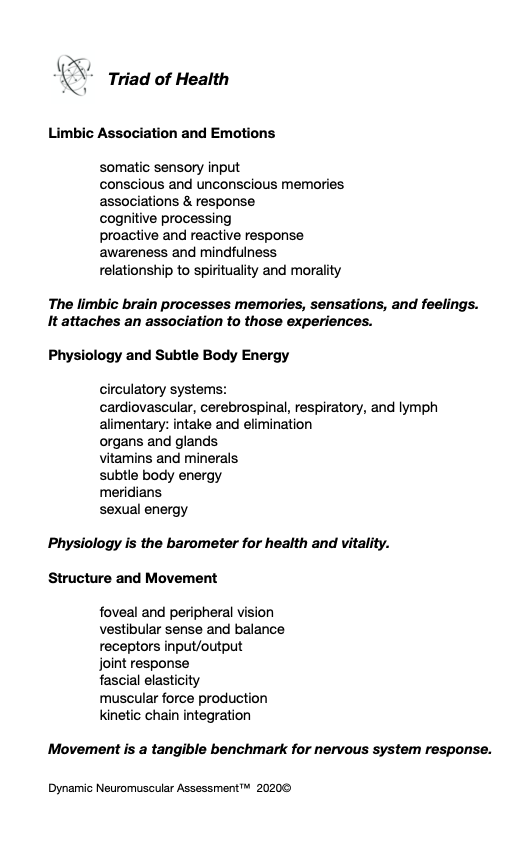
The nervous system has a full palette of options it can utilize as a prime driver at the time of the event. It can be structural, physiological, or limbic . Likewise, the nervous system can choose a main pair and subsequent secondaries from the same palette. This pallet is generalized in the Triad of Health chart.
Good Intentions – Wrong Approach
One of the common problems to recognize in the assessment and treatment of the musculoskeletal and its corresponding motor control systems is that therapists are frequently treating the symptoms. This is problematic because often those symptoms are being recruited by the nervous system for a reason. Without adequately vetting why those symptoms are present, we can inadvertently remove a necessary coping strategy. This can create vulnerability in our client’s nervous system. When we apply the universal principle of reciprocal partnership, we can be more efficient therapists. Instead of treating the low hanging fruit of the symptom, we can follow the symptom-causation relationship to derive the prime driver. When we appropriately address the prime driver, not only do we accomplish more in helping our client’s presentation, we are also honoring the primary coping strategy of their nervous system, keeping the container safe.
Let’s take a look at some examples of how the nervous system may choose to support a reciprocal relationship. As manual therapists we may be familiar with how joints and ligaments affect muscle response. Ligaments will act as neuromuscular switches for the muscles that would act on that ligament. When joint position is compromised by load, speed or vector, the ligaments role is to protect that joint. When a ligament becomes strained, it sends input signals to the cerebellum to inhibit the muscles that would act upon that joint/ligament. This is a non felt sense protection mechanism. The strained ligament will look for a reciprocal partnership to sustain this protective adaptation strategy.
An example can be applied to the knee. If during movement, the ACL gets stressed and the stress load is sufficient enough that the receptors are unable to return to a normal resting response, the movement that caused the knee to deviate into a position that stressed the ACL would be the event. The response to this event is the up-regulated receptor response to the cerebellum. The cerebellum then instructs the assisted muscle to inhibit as a protective strategy. Next, the nervous system looks for a reciprocal pair for the main driver, the strained ACL. Often in structure, the nervous system picks functional opposites. For example, the oblique popliteal ligament has an opposite function in the rotary capacity of the knee.
The low hanging fruit are the muscles that are inhibited. But there is a big problem if we then strengthen those muscles, as the action on the knee is going to increase the already hypertonic response of the ACL. This is treating the symptom! Instead, we need to derive the prime driver and cue that driver to its main pair. When the nervous system receives that information, the cerebellar response is normalized and the associated muscles return to normally responsive.
Prime drivers that are of the emotional association nature will often pair with an organ. The resources needed by the emotion is given up by the organ. A few classic examples are anger/liver and worry/stomach. The rub is if we remove the secondary compensations without addressing the prime driver, we are potentially weakening the ability of the prime driver to maintain its resource needs.
When we remove a coping strategy of the limbic system, the nervous system goes on alert with a sympathetic response. Further, depending on the spectrum of the association, mild to severe, this can be destabilizing and highly counter productive. In the severe spectrum, this can cause a PTSD episode. This is why we must evaluate the source and causation of the imbalance we are seeking to treat, before treating symptoms in the musculoskeletal system. This is how we move into being a master in our craft regardless of the corrective tools we deploy.
Let’s look at a Dynamic Neuromuscular Assessment™ Module One case study to further illustrate the concept of the prime driver.
Case Study: Assessment of the Breathing Apparatus
Global Skill: QiGong Posture
Visual: appears that the diaphragms move out of alignment creating a lack of integrity in the core cylinder
MMT: Functional Dysfunctional Response: Correlation to Limbic Association
Local Components:
Sacral Spinalis / multifidus – normally responsive
TVA – normally responsive
Pelvic Floor – functional dysfunctional
Vet Pelvic Floor:
Structural – L sub-occipitals TL
Vet L sub-occipitals – functional dysfunctional
Structural – R jaw TL
Vet R Jaw – functional dysfunctional
Limbic Association TL- same association as the global movement association
Double Check Work:
Client TL’s the R Jaw
Retest PF and L sub-occipitals
Normal Response
Corrective:
Cue the associated movements into the nervous system (order matters)
Limbic hold on the Bennett points (cranial hold, observe the breath)
Retest: (in the same order)
PF normal response
Sub-occipitals normal response
Jaw normal response
Re-insert local components back into the Global Movement
Normally Responsive
Summary:
As body helpers, our first consideration is client’s safety — what I like to call keeping the container safe. We did this by adding stability into the system. We did not remove coping strategies which would result in creating vulnerability to the system. The old MMT paradigm would indicate that we should have released the sub-occipitals. If we would have tried to correct a dysfunctional component correlated to a limbic association, potentially the response of that limbic association would have increased. That would have resulted in harming the client!
Limbic associations can have multiple layers mirroring the template of compensations with primary and secondary/s, so we had to tone down the association so that the nervous system could appropriately respond to the environment. There may be more work needed to effect sustainable change over time. However, with one corrective, we restored movement function to all the local components and the initial global assessment. That could not have happened if we did not utilize the SAID principle, specific adaptation to imposed demand, in our assessment and correction strategy.
Great article Joseph!
Thank you!